If the lower part is affected - epileptic seizures, bradycardia, anisoreflexia. Contusion lesions in the brain stem accompany fractures of the base of the skull. They are located on the outer and paraventricular surface of the brain stem, arise as a result of the application of traumatic force to various parts of the cranial vault and are formed when the trunk hits the bony protrusions and the edge of the cerebellar tentorium at the time of displacement and deformation of the brain. The small size of contusion lesions is revealed only by examining a series of sections. The ventral surface of the pons is injured by the clivus, the edge of the foramen magnum and the edge of the cerebellar tentorium. Internal contusion lesions arise due to deformation and rotation of the trunk at the time of injury in the impact zone when the brain is displaced. They are localized in the wall of the lower part of the 3rd ventricle (on the border with the Sylvian aqueduct), as well as in the remaining parts of the bottom and the area of the pen, the 4th ventricle, which is explained by the hydrodynamic mechanism from the impact of the cerebrospinal fluid wave. Foci of damage in the brain stem, outside of connection with the walls of the ventricles, appear from rotatory movements of the brain in the cranial cavity and torsion of the brain stem sections. Hemorrhages in the brain stem in the form of plaques or streaks occur as a result of displacement and impact of the brain on the basal parts of the occipital bone. It is important to distinguish primary traumatic changes at the time or in the first minutes of injury from secondary ones that form in the post-traumatic period due to cerebrovascular accident.
Cerebrovascular accident in the brain stem
A brainstem stroke is an acute disruption of blood circulation in this area, which is accompanied by the sudden onset of symptoms of neurological deficit that last longer than a day.
In Russia, the incidence rate is 3.3 per 1000 population per year, with most of them being people over 70 years of age. Mortality within the first month from the onset of the disease is 15-25%, and 70% of victims receive disability.
Thanks to the development of medicine, in recent years there has been a trend towards a decrease in the incidence and mortality from strokes. However, there is a “rejuvenation” of this disease.
Most often, stroke strikes older people, but thanks to the development of medicine, mortality is decreasing
To understand what symptoms will occur with this lesion, you need to understand what the anatomical features of the brain stem are.
A little about the structure
Brain structure
Brain stem structure
- connects brain structures.
Functions of the medulla oblongata:
Bridge functions:
Functions of the midbrain:
Etiology
Types of brainstem stroke
Causes of ischemic stroke
One of the causes of ischemic stroke is high blood pressure
Anatomy of ischemic stroke
Symptoms
Medulla
Midbrain
Diagnostics
Treatment
If you suspect a stroke, seek medical attention
Consequences
Unfortunately, brainstem stroke often has an unfavorable prognosis. The patient remains with dizziness, speech and swallowing disorders, muscle paralysis of various locations and functions, and loss of sensitivity for a long time.
Rehabilitation aimed at replacing these functions is long-term and permanent, and the improvements that occur are slow and insignificant.
However, this does not mean that you need to give up rehabilitation. Recovery is possible only by working on impaired functions.
- Tatyana on Prognosis after a stroke: how long will life be?
- Musaev on Duration of treatment for meningitis
- Yakov Solomonovich on Consequences of stroke for life and health
Copying site materials is prohibited! Reprinting of information is permitted only if an active indexed link to our website is provided.
Brain contusion: consequences and rehabilitation
Brain contusion (brain contusion) is a type of brain damage that occurs as a result of traumatic brain injury (TBI). Depending on the type and severity of the injury, pathological changes during a bruise can be varied: from single to multiple, affecting vital structures. Manifestations of brain tissue contusion are detected in 10% of victims. This pathological condition, depending on the nature of the damage and clinical manifestations, can be mild, severe or moderate.
Minor bruise GM
Due to the impact of a traumatic factor, the patient loses consciousness. This condition usually lasts for several minutes. After regaining consciousness, complaints of dizziness, repeated vomiting, nausea and headache appear. Characterized by amnesia and mild neurological symptoms (meningeal symptoms, clonic nystagmus, slight anisocoria, etc.). Breathing and body temperature do not change significantly; blood pressure and heart rate may increase. Within 3 weeks the patient recovers and the symptoms disappear.
Moderate bruise GM
The clinical picture is characterized by a loss of consciousness for a longer period (up to several hours). The patient experiences repeated vomiting, intense headache, more severe amnesia and mental disorders. An increase in blood pressure and body temperature, increased respiration, pulse, and meningeal signs are detected. Focal neurological symptoms appear, the manifestations of which depend on the location of the injury. These may be speech disorders, motor disorders (paresis), oculomotor disorders, etc. The condition improves within 3-5 weeks, focal symptoms may persist longer. During examination, damage to the skull bones and subarachnoid hemorrhage are often diagnosed. The latter develops as a result of rupture of the vessels of the pia mater, and sometimes rupture of the cerebral sinuses. Its manifestations can occur acutely (severe headache, agitation, delirium, disorientation, back pain and radicular symptoms) or increase gradually.
Severe bruise GM
After a traumatic injury, consciousness is turned off for an even longer period, which can last for days (and sometimes even weeks). Patients develop motor agitation and various neurological manifestations: impaired swallowing, paresis, paralysis, inhibition of tendon reflexes, changes in muscle tone, convulsions, multiple nystagmus, gaze paresis, pathological reflexes, etc. Examination reveals massive subarachnoid hemorrhage and skull fractures. This condition is accompanied by high temperature, increased blood pressure, and disturbances in the frequency and rhythm of breathing. General cerebral and focal symptoms slowly undergo reverse development and do not completely disappear.
Long-term consequences of bruise
- Post-traumatic encephalopathy.
- Episyndrome.
- Mental disorders.
- Residual neurological symptoms (motor, sensory, speech disorders, etc.).
Diagnostics
To recognize the severity of damage and its nature in traumatic brain injury, an integrated approach is needed. Dynamic observation plays an important role, since the patient’s condition can change quickly. When making a diagnosis, the fact of injury, duration of loss of consciousness, clinical manifestations, data from a neurological examination and additional research are taken into account. To obtain complete information about the state of the brain, the following examination methods are used:
- computer and magnetic resonance imaging (detects areas of contusion, hemorrhage, allows you to assess their size and character, as well as the condition of the ventricles of the brain, etc.);
- radiography of the skull (detects cracks and fractures of bone tissue);
- echoencephalography (determines the displacement of brain structures);
- lumbar puncture and examination of the cerebrospinal fluid (allows to recognize subarachnoid hemorrhage and intracranial hypertension, cannot be performed if there is a threat of wedging of the brain stem into the foramen magnum).
Treatment
After an injury, patients receive first aid at the scene of the accident by an emergency medical team. If the patient is unconscious, he is turned on his side or face down. First aid measures are aimed at preventing aspiration of vomit and clearing the airways, stopping bleeding. Such patients are required to be hospitalized in a hospital.
The nature and scope of treatment is determined by the condition and age of the victim, the severity of edema of brain tissue, liquor hypertension, impaired cerebral hemodynamics, etc.
All patients with a bruise of brain tissue are advised to rest, bed rest for a period of 7 days to 2 weeks, constant medical supervision is required. Drug therapy includes the prescription of the following medications:
- analgesics (ibuprofen, analgin, ketorol);
- antiemetic drugs (metoclopramide, domperidone);
- sedatives (phenazepam, Relanium, adaptol);
- with severe agitation - haloperidol, sodium hydroxybutyrate;
- diuretics (furosemide, diacarb, manitol);
- antihistamines (tavegil, suprastin);
- hemostatic agents for hemorrhage (dicinone, etamsylate);
- Medicines that improve blood circulation in brain tissue (sermion, vinpocetine);
- metabolic agents (piracetam, cerebrolysin);
- nootropic drugs (zncephabol, nootropil);
- B vitamins (milgamma, neirovitan).
To sanitize the cerebrospinal fluid and reduce its pressure, a therapeutic lumbar puncture is used.
Severe bruises of the brain require resuscitation and intensive care.
Surgical treatment is indicated for large areas of tissue crushing and the absence of effect from conservative treatment.
Measures for caring for patients with bruises of the brain consist of the prevention of bedsores, pneumonia, and passive exercises to prevent contractures.
Patients who have suffered a brain injury are subject to long-term follow-up. During the recovery period, they are recommended to take courses of vascular therapy, exercise therapy, physiotherapeutic and sanatorium-resort treatment. The latter can be prescribed several months after the injury in the absence of pronounced motor and mental disorders. In the presence of gross residual defects, the issue of the patient’s ability to work is resolved.
Physiotherapeutic treatment
To improve blood circulation in the brain tissue, the following are prescribed:
- transcerebral UHF therapy;
- medicinal electrophoresis with drugs that improve metabolism;
- laser treatment;
- air baths.
In order to reduce high cerebrospinal fluid pressure, low-intensity decimeter therapy and therapeutic sodium chloride baths are prescribed.
To improve the rheological properties of blood, laser irradiation is performed.
Conclusion
GM injury has serious consequences for human health. In severe cases, it can lead to death or disability. The most dangerous are damage to the brain stem and subcortical structures. Patients who have suffered a TBI and suffered a brain contusion must undergo long-term rehabilitation, be observed by a specialist and follow medical recommendations.
Neurologist M. M. Shperling talks about traumatic brain injury:
School of Dr. Komarovsky, section “Emergency Care”, issue on the topic “Head Injuries in a Child”:
Trunk stroke: types (ischemic, hemorrhagic), causes, symptoms, treatment, prognosis
Brainstem stroke is considered one of the most severe forms of brain damage due to acute disturbance of blood flow. This is no coincidence, because it is in the trunk that the main life support nerve centers are concentrated.
Among patients with brain stem stroke, elderly people predominate, having the corresponding prerequisites for impaired blood flow - hypertension, atherosclerosis, pathology of blood clotting, heart disease, predisposing to thromboembolism.
The brain stem is the most important area, serving as a link between the central nervous system, spinal cord and internal organs. It controls the functioning of the heart, respiratory system, maintaining body temperature, motor activity, regulates muscle tone, autonomic reactions, balance, sexual function, participates in the functioning of the organs of vision and hearing, ensures chewing, swallowing, and contains fibers of taste buds. It is difficult to name a function of our body that would not involve the brain stem.
brain stem structure
The stem structures are the most ancient and include the pons, medulla oblongata and midbrain, sometimes also including the cerebellum. In this part of the brain, the nuclei of the cranial nerves are located and conductive motor and sensory nerve pathways pass. This section is located under the hemispheres, access to it is extremely difficult, and with swelling of the trunk, its displacement and compression quickly occurs, which are fatal for the patient.
Causes and types of brainstem strokes
The causes of brainstem stroke do not differ from those in other localizations of blood flow disorders in the central nervous system:
- Arterial hypertension, which causes irreversible changes in the arteries and arterioles of the brain, the walls of blood vessels become brittle and sooner or later they may rupture with hemorrhage;
- Atherosclerosis, observed in the vast majority of older people, leads to the appearance of fatty plaques in the arteries supplying the brain, the result is plaque rupture, thrombosis, vessel blockage and necrosis of the medulla;
- Aneurysms and vascular malformations cause strokes in young patients without concomitant pathology or in combination with it.
To a large extent, the development of trunk stroke is promoted by diabetes and other metabolic disorders, rheumatism, heart valve defects, blood clotting disorders, including when taking blood-thinning drugs, usually prescribed to cardiac patients.
Depending on the type of damage, brain stem stroke can be ischemic or hemorrhagic. In the first case, a focus of necrosis (infarction) is formed, in the second, blood spills into the brain tissue when a blood vessel ruptures. An ischemic stroke has a more favorable course, but with a hemorrhagic stroke, edema and intracranial hypertension quickly increase, so mortality is much higher in the case of hematomas.
Video: basic about types of stroke - ischemic and hemorrhagic
Manifestations of brainstem damage
A brainstem stroke is accompanied by damage to the pathways and nuclei of the cranial nerves, and is therefore accompanied by rich symptoms and severe disorders of the internal organs. Signs of the disease manifest themselves acutely, starting with intense pain in the occipital region, impaired consciousness, paralysis, dizziness, tachycardia or bradycardia, and sudden fluctuations in body temperature.
General cerebral symptoms are associated with increased intracranial pressure; they include nausea and vomiting, headache, impaired consciousness and even coma. Then symptoms of damage to the nuclei of the cranial nerves and focal neurological symptoms appear.
Ischemic brainstem stroke is manifested by a variety of alternating syndromes and signs of involvement of the cranial nerve nuclei of the side where necrosis occurred. In this case, the following may be observed:
- Paresis and paralysis of muscles on the side of the affected part of the trunk;
- Deviation of the tongue towards the affected side;
- Paralysis of the part of the body opposite to the lesion with preservation of the work of the facial muscles;
- Nystagmus, imbalance;
- Paralysis of the soft palate with difficulty breathing, swallowing;
- Drooping of the eyelid on the side of the stroke;
- Paralysis of the facial muscles on the affected side and hemiplegia of the opposite half of the body.
This is only a small part of the syndromes accompanying brainstem infarction. With small lesion sizes (up to one and a half centimeters), isolated disturbances in sensitivity, movements, central paralysis with pathology of balance, hand dysfunction (dysarthria), isolated disturbance in the functioning of the muscles of the face and tongue with speech disorder are possible.
With hemorrhagic brainstem stroke, symptoms increase rapidly; in addition to motor and sensory disorders, intracranial hypertension is clearly manifested, consciousness is impaired, and the likelihood of coma is high.
Signs of hemorrhage in the trunk may be:
- Hemiplegia and hemiparesis - paralysis of the muscles of the body;
- Visual impairment, gaze paresis;
- Speech disorder;
- Decreased or absent sensitivity on the opposite side;
- Depression of consciousness, coma;
- Nausea, dizziness;
- Increased body temperature;
- Impaired breathing and heart rhythm.
A stroke usually occurs suddenly and can be witnessed by loved ones, colleagues or passers-by on the street. If a relative suffers from hypertension or atherosclerosis, then a number of symptoms should alert relatives. Thus, sudden difficulty and incoherence of speech, weakness, headache, inability to move, sweating, fluctuations in body temperature, palpitations should be a reason to immediately call an ambulance. A person’s life may depend on how quickly others orient themselves, and if the patient is admitted to the hospital in the first few hours, the chances of saving a life will be much greater.
Sometimes small foci of necrosis in the brain stem, especially those associated with thromboembolism, occur without a sharp change in condition. Weakness gradually increases, dizziness appears, gait becomes uncertain, the patient experiences double vision, hearing and vision decrease, and eating becomes difficult due to choking. These symptoms also cannot be ignored.
Trunk stroke is considered a severe pathology, and therefore its consequences are very serious. If in the acute period it is possible to save life and stabilize the patient’s condition, bring him out of a coma, normalize blood pressure and breathing, then significant obstacles arise at the rehabilitation stage.
After a brainstem stroke, paresis and paralysis are usually irreversible, the patient cannot walk or even sit, speech and swallowing are impaired. There are difficulties with eating, and the patient needs either parenteral nutrition or a special diet with liquid and pureed food.
Contact with a patient who has suffered a brainstem stroke is difficult due to speech impairment, but intelligence and awareness of what is happening can be preserved. If there is a chance to at least partially restore speech, then a specialist aphasiologist who knows techniques and special exercises will come to the rescue.
After a heart attack or hematoma in the brain stem, patients remain disabled, requiring constant participation and assistance in eating and performing hygiene procedures. The burden of care falls on the shoulders of relatives, who must be aware of the rules of feeding and handling a seriously ill person.
Complications from brainstem stroke are not uncommon and can cause death. The most common cause of death is considered to be edema of the brainstem with its entrapment under the dura mater of the brain or in the foramen magnum; uncorrectable disturbances of the heart and breathing, and status epilepticus are possible.
In a later period, urinary tract infections, pneumonia, thrombosis of the leg veins, and bedsores occur, which is facilitated not only by neurological deficits, but also by the forced recumbent position of the patient. Sepsis, myocardial infarction, and bleeding in the stomach or intestines cannot be ruled out. Patients with milder forms of brainstem stroke who attempt to ambulate are at high risk of falls and fractures, which can also be fatal.
Relatives of patients with brain stem stroke already in the acute period want to know what the chances of recovery are. Unfortunately, in a number of cases, doctors cannot reassure them in any way, since with this localization of the lesion we are talking about saving lives in the first place, and if the condition can be stabilized, then the vast majority of patients remain deeply disabled.
The inability to correct blood pressure, high, persistent body temperature, and a comatose state are unfavorable prognostic signs in which there is a high probability of death during the first days and weeks after the onset of the disease.
Treatment of brainstem stroke
Trunk stroke is a serious, life-threatening condition that requires immediate treatment; the prognosis of the disease largely depends on how quickly treatment is started. All patients, without exception, must be hospitalized in specialized departments, although in some regions this figure is terribly small - about 30% of patients are admitted to hospital on time.
The optimal time to start treatment is considered to be the first 3-6 hours from the onset of the disease, while even in large cities with high availability of medical care, treatment is often started after 10 or more hours. Thrombolysis is performed on a few patients, and round-the-clock CT and MRI scans are more a fantasy than a reality. In this regard, forecast indicators continue to remain disappointing.
A patient with a brainstem stroke should spend the first week in the intensive care unit under the constant supervision of specialists. When the acute period is over, transfer to the early rehabilitation ward is possible.
The nature of therapy has specific features for ischemic or hemorrhagic types of lesions, but there are some general principles and approaches. Basic treatment is aimed at maintaining blood pressure, body temperature, lung and heart function, and blood constants.
To maintain lung function you need:
- Sanitation of the upper respiratory tract, tracheal intubation, artificial ventilation;
- Oxygen therapy for low saturation.
The need for tracheal intubation during a brainstem stroke is associated with impaired swallowing and cough reflex, which creates the preconditions for stomach contents to enter the lungs (aspiration). Blood oxygen is monitored using pulse oximetry, and its oxygen saturation (saturation) should not be lower than 95%.
When the brain stem is damaged, there is a high risk of cardiovascular disorders, so the following is necessary:
Even for those patients who did not suffer from arterial hypertension, antihypertensive drugs are indicated to prevent recurrent stroke. In addition, if the pressure exceeds 180 mm Hg. Art., the risk of worsening brain disorders increases by almost half, and a poor prognosis by a quarter, which is why it is so important to constantly monitor blood pressure.
If the pressure was high before the brain damage, then maintaining it at a level of 180/100 mmHg is considered optimal. Art., for people with initial normal blood pressure – 160/90 mm Hg. Art. Such relatively high numbers are due to the fact that when pressure drops to normal, the degree of blood supply to the brain also decreases, which can aggravate the negative consequences of ischemia.
To correct blood pressure, labetalol, captopril, enalapril, dibazol, clonidine, and sodium nitroprusside are used. In the acute period, these drugs are administered intravenously under pressure control, and later oral administration is possible.
Some patients, on the contrary, suffer from hypotension, which is very detrimental to the affected part of the brain, because hypoxia and neuronal damage increase. To correct this condition, infusion therapy with solutions (reopolyglucin, sodium chloride, albumin) is carried out and vasopressors are used (norepinephrine, dopamine, mesaton).
Monitoring of biochemical blood constants is considered mandatory. So, when the sugar level decreases, glucose is administered, and when the sugar level increases by more than 10 mmol/l, insulin is administered. In the intensive care unit, sodium levels, blood osmolarity, and the amount of urine excreted are constantly measured. Infusion therapy is indicated when the volume of circulating blood decreases, but at the same time, a slight excess of diuresis over the amount of infused solutions is allowed as a measure to prevent cerebral edema.
Almost all patients with brain stem strokes have an elevated body temperature, because the thermoregulation center is located in the affected part of the brain. The temperature should be reduced starting from 37.5 degrees, for which paracetamol, ibuprofen, and naproxen are used. A good effect is also obtained by injecting magnesium sulfate into a vein.
The most important stage in the treatment of brain stem stroke is the prevention and control of cerebral edema, which can lead to displacement of the midline structures and their wedging into the foramen magnum, under the tentorium of the cerebellum, and this complication is accompanied by high mortality. To combat cerebral edema, use:
- Osmotic diuretics – glycerin, mannitol;
- Administration of albumin solution;
- Hyperventilation during mechanical ventilation;
- Muscle relaxants and sedatives (pancuronium, diazepam, propofol);
- If the measures listed above do not bring results, barbiturate coma and cerebral hypothermia are indicated.
In very severe cases, when it is not possible to stabilize intracranial pressure, muscle relaxants, sedatives and artificial ventilation are used simultaneously. If this does not help, surgical intervention is performed - hemicraniotomy aimed at decompressing the brain. Sometimes the ventricles of the brain are drained - in case of hydrocephalus with an increase in pressure in the cranial cavity.
Symptomatic therapy includes:
- Anticonvulsants (diazepam, valproic acid);
- Cerucal, motilium for severe nausea, vomiting;
- Sedatives – Relanium, haloperidol, magnesia, fentanyl.
Specific therapy for ischemic stroke consists of thrombolysis, the administration of antiplatelet agents and anticoagulants to restore blood flow through the thrombosed vessel. Intravenous thrombolysis should be carried out in the first three hours from the moment of blockage of the vessel; alteplase is used.
Antiplatelet therapy consists of prescribing aspirin; in some cases, the use of anticoagulants (heparin, fraxiparin, warfarin) is indicated. To reduce blood viscosity, it is possible to use rheopolyglucin.
All of the listed methods of specific therapy have strict indications and contraindications, so the advisability of their use in a particular patient is decided individually.
Neuroprotective therapy is needed to restore damaged brain structures. For this purpose, glycine, piracetam, encephabol, cerebrolysin, emoxypine and others are used.
Specific treatment of hemorrhagic strokes consists of the use of neuroprotectors (mildronate, emoxipine, Semax, nimodipine, actovegin, piracetam). Surgical removal of the hematoma is difficult due to its deep location, but stereotactic and endoscopic interventions have advantages, minimizing surgical trauma.
The prognosis for a brainstem stroke is very serious, the mortality rate for heart attacks reaches 25%, and with hemorrhages, more than half of the patients die by the end of the first month. Among the causes of death, the main place belongs to cerebral edema with displacement of stem structures and their infringement in the foramen magnum, under the dura mater. If it is possible to save the life and stabilize the patient’s condition, then after a brainstem stroke he will most likely remain disabled due to damage to vital structures, nerve centers and pathways.
Brain stem hemorrhage prognosis
The brainstem is important for the normal functioning of the body. It is in this part of the brain that there are formations that are responsible for breathing and blood circulation, in addition, it is in this part of the brain that the axons of the craniofacial nerves are located.
A brainstem stroke paralyzes the functioning of this organ, so a person’s functioning of vital organs is disrupted. Such damage most often leads to the death of a person, but with prompt medical assistance there is a possibility of a successful outcome.
If a person who has suffered a stroke remains alive, his mobility and other functions are restored quite slowly after long-term therapy.
It is worth remembering that although the functions of the body will not be fully restored after a stroke, you can still expect some improvement in the condition of the human body with proper treatment.
What happens to the body during a stroke?
In normal condition, the blood vessels of the human body are quite elastic and strong. However, with constant load on them at high pressure, their walls become thinner and become quite fragile. After another hypertensive crisis, the vessels cannot withstand it and burst.
Hemorrhage occurs in the human brainstem. the resulting hematoma blocks the access of oxygen to this part of the brain. Lack of oxygen leads to the fact that the brainstem atrophies, ceasing to ensure the coordinated functioning of vital internal organs.
Treatment of brainstem stroke
Brainstem stroke is quite difficult to treat. Quite long-term and professional treatment is required, which includes inpatient treatment and physical therapy. In severe cases, emergency surgery may be required.
In the first few hours after a stroke, surgery is necessary to stop the bleeding.
However, a brainstem stroke most often occurs so severely that it does not allow the use of angiographic examination or any other surgical intervention. In this case, the necessary resuscitation measures are applied.
Recently, there has been a focus on reinfusing patients' platelets at the site of injury. Research and medical practice have shown the effectiveness of this method, especially in the first hours after a stroke.
Statistics show that patients who underwent such therapy experienced an improvement in the recovery process of ischemic neurons.
Mortality among such patients also decreased markedly, and damage to the body's motor functions became much less. In addition, the use of this method reduced the risk of late complications.
In the first days after a stroke, the patient is treated in a hospital. In addition to tests that reveal the extent of damage to the brainstem, therapy is prescribed that pursues the following goals:
- support all important body functions;
- minimize physical and emotional stress on the body;
- relieve inflammation and swelling of damaged areas of the brain and restore normal blood supply to areas of the brain located in the stroke area;
- restore blood functions especially in relation to coagulation and its viscosity;
- maintaining normal functioning of the cardiovascular system;
- specific treatment prescribed depending on the degree and size of the lesion.
During the first weeks, treatment for a patient who has suffered a brainstem stroke may include, in addition to medication, physical exercise.
During this period of time, coordination of the efforts of specialist doctors in various fields is very important in coordinating medication treatment, rehabilitation of the patient and his education.
As a medicinal treatment during this period, drugs are used that take on the role of transmitting impulses from nerve cells in the brain, helping to restore normal functioning of brain functions.
A short time after the stroke and during the first months, rehabilitation therapy is carried out. The effectiveness of such therapy in the first months of treatment has been proven by many studies and results.
You should not postpone such therapy until a later time, because the brain acquires a permanent loss of certain brain functions that are practically not restored.
Rehabilitation therapy can be carried out not only at home or in rehabilitation centers. You can also use the help of specialized sanatoriums.
Treatment prognosis
As already noted, treatment for brainstem stroke is quite difficult and slow. Therefore, with a brain stem stroke, the prognosis of treatment largely depends on how quickly treatment of the disease began and also on the degree of brain damage.
If a patient has experienced an ischemic stroke of the brain, then in 60% of cases this is followed by death within the first months; a hemorrhagic stroke is more severe and in its case the mortality rate reaches 80%.
With timely, qualified medical care, the mortality rate is sharply reduced. Therefore, timely detection of disease symptoms and early diagnosis can reduce the risk of death and the consequences of stroke.
Of all those who have suffered an ischemic stroke, only 20% of people will be able to fully restore body functions. During the first thirty days, 8-82% of patients die, depending on the type of stroke. But again, everything depends on the provision of qualified assistance and the degree of brain damage.
The most dangerous factor of the disease is that a recurrence of stroke is possible in the first months after the first incident occurred. Exacerbations associated with the condition of the brain in the second case are more serious than in the first, so mortality after the second stroke is almost 100%.
Depending on the type of stroke and how quickly help was provided, a prognosis for the patient’s recovery can be made. A brainstem stroke most often has irreversible consequences, proceeds quite violently and causes damage that leads to death or disability. Full recovery from this type of stroke is almost impossible.
Understanding the serious consequences of a stroke and how difficult the rehabilitation course is, it is worth making additional efforts to ensure that the patient’s close relatives, as well as the person at risk, can detect the symptoms of a stroke in the early stages and consult a doctor in a timely manner.
A little about the structure
The brain consists of the cerebral hemispheres and the brainstem.
The structure of the trunk includes the medulla oblongata, midbrain, diencephalon, and pons.
It performs the following functions:
- provides reflexive behavioral activity;
- connects the upper and lower parts of the central nervous system via conductive pathways;
- connects brain structures.
The composition includes gray and white matter. Gray – neurons located in the form of nuclei that have specific functions. White – conductive paths. To distinguish a stroke in the brain stem from others, as well as to accurately determine the location of the lesion, you need to understand the functions of its parts.
Functions of the medulla oblongata:
- Innervation of the muscles of the tongue (nucleus of the XII pair of cranial nerves) and some muscles of the head (nucleus of the XI pair), larynx and oral cavity (nucleus of the IX pair).
- The work of the parasympathetic nervous system (vagus nerve - X pair).
- Maintaining vital functions (breathing, heartbeat) is the core of the reticular formation.
- The implementation of some motor functions is carried out by the extrapyramidal nuclei (oliva).
Bridge functions:
- Conduction of auditory impulses (nuclei of the VIII nerve).
- Providing facial movements, as well as tear and salivation (nuclei of the VII nerve).
- Carrying out the abduction of the eye outwards (nuclei of the VI pair).
- Chewing movements are carried out by the nuclei of the V pair of cranial nerves.
Functions of the midbrain:
- Other movements of the eyeball, eyelids, pupil (IV and III pairs of nerves).
- Regulation of muscle movement and tone (nucleus of the substantia nigra).
- Reflex response to light and sound impulses.
- Muscle sensitivity of the face and neck.
- Coordination of joint rotation of the neck and eyes.
- Collection of sensitive information from internal organs.
The brain stem coordinates the work of all internal organs, reflex activity, and some important motor acts. Depending on the location of the lesion, symptoms will vary.
Etiology
By origin, brainstem stroke occurs:
- ischemic is associated with a lack of blood flow due to blockage (obstruction) of the artery supplying the area;
- hemorrhagic due to rupture of the artery and bleeding from it.
The first type is much more common than the second, accounting for 75-80% of all cerebrovascular accidents.
Causes of ischemic stroke
Risk factors for ischemic stroke include old age, high blood pressure, increased cholesterol in the blood, atherosclerosis, smoking, heart disease, and diabetes.
It should be noted that the increase in blood pressure is above 140/90 mm. Hg, relative to normal, doubles the risk of stroke.
All causes of ischemic stroke can be divided into groups:
- Atherothrombotic - ischemia occurs due to a slowly increasing plaque in the area of the vessel. Such a stroke is preceded by symptoms of transient cerebrovascular accident, signs of prolonged “robbing” the brain of oxygen and nutrients: memory loss, absent-mindedness, development of tearfulness or irascibility, and others. More often happens at night or early in the morning.
- Embolic develops suddenly; a sharp and rapid blockage of the afferent artery occurs with an embolus. More often it occurs with heart diseases (atrial fibrillation, defects, artificial valves), which are characterized by the formation of blood clots in the cavities of the heart and their spread through the bloodstream. More often happens during the day, during emotional or physical overload.
- Ischemia may develop with a decrease in blood pressure, when there is insufficient blood flow to the brain. This is a hemodynamic type.
- Lacunar is characterized by damage to small arteries located deep in the brain. It often develops during the day, against the background of high blood pressure. Since small areas are deprived of blood supply, the symptoms are erased, and its prognosis is better than that of others.
- Hemorheological is rare and develops due to increased blood viscosity.
The brain is an organ where chemical processes actively occur, but it does not have its own reserves of nutrients. This means that any reduction in blood flow with oxygen and nutrients quickly affects its function in a negative way. Without a blood supply, a neuron can survive for a maximum of five to eight minutes, after which it dies.
Normally, ml of blood flows through 100 g of brain per minute; with a stroke, this figure drops to 10.
After blockage of a vessel, the following is possible: ischemia occurs in the area it fed, neurons die, and their function is lost. But next to it there is another area (ischemic penumbra or penumbra), in which the blood supply has not reached a dangerous minimum. However, the brain cells in it also suffer from ischemia and damage from the decay products of dead neurons. They are viable, but they are also at risk of death, so it is important to start therapy as early as possible. This will reduce the affected area and preserve more brain functions.
Due to the accumulation of breakdown products, edema develops in this area, which compresses adjacent structures, pushing them to the side, further impairing blood flow and functioning.
Causes of hemorrhagic stroke
It occurs less frequently, but its symptoms are more severe and the prognosis is worse. Highlight:
- With parenchymal hemorrhage, changes occur in the substance of the brain. This is possible with arterial hypertension, bleeding disorders or weakness of the vascular wall (aneurysm).
- Subarachnoid - bleeding onto the surface of the brain due to pathology of the vessels in the membranes. More often, it is caused by an aneurysm, so it usually affects young, apparently healthy people.
A brainstem stroke develops when there is a lesion in the vertebrobasilar vascular system.
Symptoms
Brainstem stroke manifests itself in different ways, depending on the location of the lesion. It is characterized by the appearance of alternating (cross) symptoms, that is, the organs of the head and neck are affected on the side of the lesion, and the movements of the limbs and the sensitivity of the skin of the body are affected on the opposite side.
Medulla
If the medulla oblongata is damaged, there will be a complete or partial impairment of the motor function of the tongue (its tip deviates in the direction of the lesion), the muscles of the soft palate, neck, vocal cords (hoarseness) on the side of the stroke, and loss of sensitivity of the facial skin. On the opposite side there is a violation or inability to move the arms or legs, numbness of half the body.
Stroke has a poor prognosis in the presence of bulbar palsy. It develops when blood circulation in the vertebral arteries is impaired, which causes bilateral damage to the IX, X, XII pairs of cranial nerves located in the medulla oblongata. In this case, such disorders as choking when swallowing, overhanging soft palate, impaired diction, hoarseness of voice, small twitching of the tongue and limited mobility are noted. It is often followed by impairment of vital functions and death.
If the pathological focus is in the bridge, then on the affected side there is an inability to move the facial muscles, loss of superficial sensitivity on the face, decreased hearing, the gaze is directed towards the focus. On the opposite side, motor disturbances in the limbs and decreased sensitivity are detected. Often accompanied by impaired consciousness up to coma.
Pseudobulbar palsy manifests itself in the same way as bulbar palsy, but its cause is damage to the pathways at the level of the pons and above, so the prognosis is more favorable, since disturbances in vital functions usually do not follow. A distinctive feature is the absence of tongue twitching, the pharyngeal and palatal reflexes are preserved or increased, and symptoms of oral automatism are detected.
With thrombosis of the basilar artery, “locked-in syndrome” develops. While consciousness is preserved, the patient does not move any muscles except the eyeballs and blinking.
Midbrain
A brainstem stroke localized in the midbrain is manifested by the inability to make eye movements and lack of pupillary response on the affected side. On the opposite side, the movement of the limbs is disrupted, and tremor (involuntary shaking) of the hand appears. Pseudobulbar palsy may develop.
Decerebrate and decortication rigidity syndrome indicates a poor prognosis. The cause is a brainstem stroke in the area of the midbrain pathways at a level above the vestibular nuclei. Decerebrate rigidity is manifested by coma in combination with an increase in the tone of all muscles, mainly extensors, when the arms and legs are brought to the body and the head is thrown back. Decortication - the upper limbs are bent and the lower limbs are extended.
If the lesion is localized below the vestibular nuclei, then coma occurs with a lack of muscle tone.
Diagnostics
If a brainstem stroke is suspected, as with other lesions, magnetic resonance or computed tomography is performed, if possible. This makes it possible to identify the presence and location of an area of impaired blood circulation. The speed of correct diagnosis directly affects the final prognosis of the disease.
Doppler ultrasound is a technique for studying blood flow in vessels. It identifies areas of missing blood supply or hemorrhage.
An important indicator of the functional characteristics of the body are general clinical tests (general blood and urine analysis), biochemical blood test, ECG, and, if necessary, EchoCG (visual ultrasound examination of the heart).
All this information allows us to establish the diagnosis of stroke, its localization, which determines the prognosis of recovery and treatment tactics.
Treatment
If a stroke of any localization is suspected, hospitalization in the neurological department is required.
Trunk stroke is treated according to the same principles as any other. Basic therapy includes maintaining vital body functions: breathing, blood pressure, heartbeat, body temperature, as well as reducing cerebral edema.
Specific therapy is aimed at eliminating the causes of the disease. This includes, for example, thrombolysis, normalization of blood viscosity. Measures are being taken to provide neuroprotection and restore neuronal function.
The faster the symptoms of neurological deficit pass, the better the future prognosis.
Features of the brainstem
The brainstem connects the brain and spinal cord. Through it, all commands from the brain are processed to the human body; a person’s motor ability depends on its normal functioning. If the integrity of the blood vessels in the brain stem is disrupted, changes in functioning can occur in the following areas:
These parts of the brain are responsible for breathing, blood flow, swallowing functions, facial expressions (smiling, eyelid movement, etc.) and thermoregulation.
With a brainstem stroke, many departments are threatened. A hematoma formed due to hemorrhage can stop oxygen supply to brain cells, causing them to atrophy and die.
Mechanism of the disease
According to the mechanism of action, brainstem stroke is divided into ischemic and hemorrhagic. Ischemic stroke occurs when a blood vessel becomes obstructed due to blockage by a blood clot or plaque. Hemorrhagic occurs when a vessel ruptures due to thinning.
Hemorrhagic brainstem stroke differs from ischemic stroke in the high rate of increase in symptoms. Ischemic infarction is the most dangerous because symptoms may appear so late that the patient cannot be saved.
What causes the violation
The main causes of cerebral infarction include the occurrence of blood clots and plaques in the lumen of blood vessels, as well as thinning of the walls of blood vessels. But such reasons do not appear on their own; they are a consequence of the following diseases:
- constant high blood pressure (hypertension) and its surges;
- vascular aneurysm;
- poor blood clotting;
- diseases of the cardiovascular system;
- thinning of blood vessels due to diabetes mellitus;
- high cholesterol and atherosclerosis;
- hormonal disorders that occur when taking birth control pills incorrectly.
If you have at least one disease, a person is at risk of developing a brainstem stroke.
Violation clinic
The onset of a brainstem stroke is always sudden, and some symptoms may be similar to other diseases, which complicates the correct diagnosis.
In 70% of cases when a stroke is not detected in a timely manner, death occurs immediately or after several days. Therefore, it is important to know the symptoms indicating a brainstem hemorrhage, since there are only 3 hours to help the patient.
General symptoms include:
- speech impairment: words become unclear, speech is slurred;
- headaches of varying intensity;
- dizziness;
- pallor of the face may be replaced by a rush of blood and vice versa;
- impaired eye mobility;
- the face and whole body are covered with cold sweat;
- jumps in body temperature, from very low to high;
- decreased heart rate;
- numbness of the arms and legs, inability to move, lift, or walk;
- heavy intermittent breathing, shortness of breath;
- there are no swallowing reflexes, it is impossible to even drink water;
- the face may become distorted, asymmetry may appear, the patient may squint in one eye;
- paralysis of one side of the body.
Sometimes, when the brain stem is disrupted, complete paralysis of the body can occur; a person cannot move or speak, but at the same time his mind and intelligence are clear, he understands everything - this happens very rarely. Clarity of consciousness can be indicated by even breathing and pulse, attempts to blink an eye or move your lips.
Hemorrhagic stroke develops very quickly, which allows for a timely diagnosis. Ischemic can develop from several hours to a day, and there may be mild numbness of a part of the face or body, tingling, pain in the eye, dizziness and blurred vision of one or both eyes.
The importance of timely diagnosis
After symptoms appear and first aid is provided, it is important to conduct a diagnosis to determine the areas of brain damage. It depends on how serious the consequences will be and, most importantly, how long the recovery will be.
After consultation with a neurologist, a number of examinations are prescribed:
- MRI. In case of ischemic and hemorrhagic stroke at the initial stage of development, it helps to confirm the diagnosis and stop its further development. In some cases, contrast tomography may be performed.
- Cardiography. It is used to determine whether there are changes in the heart rhythm, which may indicate a disturbance in the intensity of blood flow.
- Angiography. Detects disorders in the cardiovascular system due to atherosclerosis, thrombosis, etc.
- Cardiogram.
- General and detailed blood test.
- Ultrasound of cerebral vessels.
Basically, all stages of diagnosis occur in intensive care conditions.
First aid in a medical facility
If a brain stem stroke is confirmed, a drug is immediately administered to dissolve the blood clot that caused the blockage of the vessel.
This will restore blood flow through the vessels of the brain, which not only improves the patient’s condition, but also prevents the progression of the disease.
Then the functioning of the lungs and heart is monitored. If the patient is unconscious, breathing problems are often observed; to eliminate the problem, a breathing tube is inserted into the patient’s trachea to maintain oxygen supply.
Further therapy
Trunk stroke cannot be cured; the only thing doctors can do to save the patient’s life is to eliminate the cause of the stroke. Treatment depends on the severity of the stroke, as well as its type (ischemic or hemorrhagic).
Surgical intervention
For hemorrhagic infarction of the brainstem, the main treatment is surgery to remove the resulting hematoma.
A less traumatic operation is performed using a small hole through which a thrombolytic agent is injected to resolve the hematoma.
This type of operation is contraindicated for aneurysms and other vascular pathologies; it is well tolerated by hypertensive patients.
Drug treatment
After surgery or after drug restoration of blood flow, drug treatment is prescribed with drugs that thin the blood, control blood pressure and heart rate, and antiemetics and cholesterol-lowering drugs are also used.
Treatment of brainstem stroke is carried out using the following medications:
- Drugs that control blood pressure (Verapamil, AD Norma, Isoptin, Cordafen).
- Anticoagulants that help improve blood clotting (Thrombin, Vikasol, Fibrinogen).
- Medicines to improve metabolism and lower cholesterol (Vasilip, Ovencor, Simvastol, Sincard).
- At elevated body temperatures, antipyretics are prescribed (Diclofenac, Nurofen, Analgin).
- Hormonal drugs to restore functions impaired due to damage to the brain stem (Epithalamine).
Drug treatment helps partial recovery and is also necessary to stop the progression of the disease. In addition, massage, hirudotherapy, reflexology and acupuncture are prescribed to speed up recovery.
Consequences and prognosis
The prognosis after a brainstem stroke is disappointing. Even with timely first aid, a person often remains partially or completely paralyzed.
The main consequences of a brain stem stroke:
- speech disorders;
- violation of swallowing and respiratory functions;
- impairment of motor abilities;
- impaired coordination;
- instability of thermoregulation;
- loss of vision.
How to prevent it?
After a brain stem stroke, to prevent complications, as well as relapse or the occurrence of the disease for the first time, the following rules must be followed:
- lead a healthy lifestyle: don’t drink, don’t smoke, watch your weight;
- control pressure and prevent its surges;
- avoid stressful situations;
- systematically visit a cardiologist after 45 years;
- treat existing chronic heart and vascular diseases.
Following the rules does not guarantee that the disease will not burst into your life, but it significantly reduces the risk of its occurrence.
Mechanism of occurrence
According to the mechanism of occurrence, brainstem stroke is distinguished between hemorrhagic and ischemic. The first occurs due to a rupture of the artery supplying the brain, which leads to hemorrhage. Its cause is hypertension or congenital pathology of blood vessels, expressed in their thinning. The second type, ischemic, is characterized by blockage of the vessel caused by obstruction of the vessel due to the entry of an atherosclerotic plaque or thrombus into the lumen.
Not only the mechanism of occurrence is different, but also the course: a hemorrhagic stroke occurs instantly, while an ischemic stroke occurs gradually, its symptoms increasing.
Treatment doctors use different methods for different types of stroke. What alleviates ischemic disease can be harmful in the case of hemorrhagic disease.
Symptoms
Hemorrhagic brainstem stroke has acute symptoms. Ischemic, developing gradually, from several hours to a day, is manifested by numbness of the face or part of the body, tingling, pain in the eye, blurred vision, loss of balance. The most obvious symptoms of both types are paralysis.
If an ischemic stroke develops, the following manifestations should alert relatives and the patient himself:
- sudden pallor, redness of all or part of the face;
- difficulty and rapid breathing, sometimes with wheezing;
- impaired speech clarity;
- dizziness;
- sweating;
- decreased and tense pulse;
- temperature increase;
- increased blood pressure.
Forecast
Trunk stroke is fatal in two thirds of cases. A more favorable prognosis is possible in young patients and in cases where the patient quickly ends up in a clinic specializing in the treatment of strokes. This institution has neurologists and neurosurgeons on staff, and has special equipment - a tomograph and other devices. Ideally, a computed tomography scan is performed in the first hour of illness.
Diagnostics
Computed tomography can rule out hemorrhage. This procedure is carried out within a few seconds, the patient has time to hold his breath once, and the result is ready. If hemorrhage is excluded, magnetic resonance imaging is performed. It takes up to half an hour, but this type of research provides much more information.
If time permits, ultrasound scanning of blood vessels and angiography are performed. The information obtained allows the doctor to prescribe adequate treatment.
Treatment
For hemorrhagic stroke, the main treatment is surgery. Open craniotomy is performed to eliminate the hematoma. A less invasive method is to administer a thrombolytic through a drilled hole to promote resorption of the hematoma. The second type of surgery is contraindicated for vascular pathologies and aneurysms. It is ideal for hypertension.
The time interval allotted to prevent the terrible consequences of an ischemic stroke is several hours. During this time, it is necessary to restore blood circulation in the artery suffering from embolism. Systemic thrombolysis will allow you to survive the disease with minimal losses. For intravenous administration of drugs, several conditions must be met:
- minimum time elapsed since the onset of the disease;
- no surgery shortly before the stroke.
Consequences
Speech Impairment
In a third of patients, brainstem stroke causes speech disorders: slurred, quiet, unclear speech. Such a violation is corrected by treatment with the participation of a speech therapist.
Swallowing disorder
This sign most clearly characterizes a brainstem stroke. More than half of patients have symptoms of swallowing dysfunction (dysphagia). The prognosis for partial or complete recovery is uncertain. There are techniques that can alleviate this condition - teaching the patient to swallow soft, ground food.
Impaired motor function of the limbs
Common consequences of the disease are spontaneous, uncoordinated movements of the arms and legs. For the restoration of movements in the first two months there is a positive prognosis, later the dynamics slow down. Gradual improvements are observed throughout the year; later, recovery rarely occurs.
Loss of coordination
Dizziness is a common accompaniment of stroke, and it quickly goes away during treatment. The prognosis for complete relief from it is uncertain.
Breathing problems
The inability to breathe independently is the result of damage to the brain stem. The treatment has an unfavorable prognosis, the patient is completely dependent on the artificial respiration apparatus. If the respiratory center is not completely destroyed, patients can breathe on their own while awake, but short-term pauses in breathing are possible during sleep.
Hemodynamic instability
An unfavorable prognosis is a decrease in heart rate, which indicates the severity of the patient’s condition and the possibility of death.
Unstable thermoregulation
The severity of the consequences of a stroke is indicated by a violation of thermoregulation. On the first day after the onset of the disease, body temperature rises sharply and is difficult to correct. A significant drop in temperature, which may be a harbinger of brain cell death, also has adverse consequences.
Visual impairment
Ischemic stroke affecting the brainstem is characterized by impaired eye movements. One or both eyeballs may begin to spontaneously move in different directions, making it impossible to fixate on an object.
Therapy and rehabilitation until recovery include maintaining body functions, eliminating emotional and physical stress, relieving swelling and restoring blood circulation. The younger the patient is, the faster he is in the hands of qualified doctors, the more favorable the prognosis will be, and the less destructive the consequences.
Brainstem stroke is one of the localizations of acute pathology in the blood supply to the brain.
2 types of stroke (ischemic and hemorrhagic) have different preferential localizations. If hemorrhages often occur in the cortical structures of the brain, then ischemia develops in the brain stem. The severity of the disease is confirmed by unfavorable statistics: in 2/3 of cases, death is observed in the first two days.
Where is the brain stem located?
The brainstem is the lowest part of the brain, bordering the spinal cord. Anatomically, it is located at the base of the skull. The top and sides are covered by the hemispheres, and the cerebellum is adjacent to the back. In their structure, stem cells are more similar to spinal cord cells. Their tasks:
- ensuring the constant functioning of centers regulating and supporting cardiac activity, breathing, muscle tone and movements;
- communication between cortical centers and the spinal cord through passing nerve pathways (centripetal - from the cortical centers to the spinal cord, centrifugal - back).
There are 3 parts in the trunk.
The medulla oblongata is the lowest zone, practically a continuation of the spinal cord, containing vital centers of respiration (regulate inhalation and exhalation), blood circulation (accelerates or slows down the rhythm). Malfunction threatens a person with cessation of respiratory movements, a drop in blood pressure, cessation of cardiac activity and death. The nuclei that control coughing, sneezing, vomiting, swallowing, and blinking are also located here.
Important cranial nerves such as the vagus, glossopharyngeal, hypoglossal and accessory nerves originate from the cells of the medulla oblongata. One of the main pathways - the pyramidal one - goes from the motor centers of the cortex to the cells of the spinal cord located in formations called “anterior horns”.
The bridge - all connections of the cerebral cortex with the cerebellum, spinal cord, and the transmission of auditory information pass through it. It contains the nuclei of the trigeminal, statoacoustic, abducens and facial nerves.
Midbrain - neurons in this area regulate muscle tone, provide the possibility of movements, protective reflexes in response to visual or auditory factors, unconscious human reactions, for example, simultaneous turning of the head and eyes towards the switched on light stimulus.
What happens during a stroke?
A brainstem stroke in the form of hemorrhage can occur as an independent focus, then the bridge is most often affected. Such changes often result in a breakthrough of blood into the fourth ventricle. If small hemorrhagic lesions accompany larger damage to the hemispheres, they can merge and aggravate the general neurological symptoms.
Ischemic processes in brain tissue are associated with impaired blood flow through the anterior, middle and posterior cerebral arteries or through external feeding vessels (internal carotid, vertebral). The formation of an infarction zone during a brainstem stroke is accompanied by swelling of the brain tissue, which compresses the nerve trunks and centers, causing venous congestion and hemorrhage.
As a result, brain volume increases and intracranial pressure increases. This promotes the displacement of various brain structures. When part of the medulla oblongata is wedged and pinched in the foramen magnum of the skull, the patient’s condition is extremely serious and ends in death. Such consequences make the main task in stroke therapy the fight against edema and the administration of diuretics in the first hours of the disease.
Causes
The causes of brainstem stroke do not differ from cerebrovascular accidents of other locations:
- atherosclerosis of arteries;
- diabetes;
- hypertension;
- rheumatic vasculitis.
Hereditary predisposition affects the regulation of vascular tone, impaired structure of vascular walls, and metabolic changes in brain tissue.
Clinical manifestations
Hemorrhage into the brain stem is characterized by:
- sharp constriction of the pupils;
- drooping eyelid (ptosis) on the side of the lesion;
- floating movements of the eyeballs;
- cranial nerve palsy;
- rapid development of pneumonia with a tendency to edema;
- breathing type disorder (Cheyne-Stokes);
- paralysis of the limbs on the opposite side to the lesion;
- high blood pressure;
- comatose state;
- increased body temperature;
- wet skin on the affected side due to increased sweating.
Ptosis of the right eyelid indicates a lesion in the right half of the trunk
Trunk ischemia, thrombotic or non-thrombotic, often occurs gradually. Damage to the area of the vertebral and basilar arteries is more typical. All signs alternate between periods of improvement and deterioration, but the disease is steadily progressing. The patient is concerned about:
- dizziness;
- staggering when walking;
- decreased hearing and vision;
- double vision;
- speech disorder (scanning phrases).
If a heart attack develops in the affected area, the following signs appear:
- paralysis of half the body with impaired sensitivity;
- impairment of the patient's consciousness to the point of coma;
- change in breathing (rare with wheezing), rapid onset of pneumonia.
Alternating syndromes in the stroke clinic
A brainstem stroke differs from impaired blood circulation in the cerebral cortex by the involvement of the nuclei and pathways of the motor nerves. Therefore, patients have a combination of central paralysis with peripheral manifestations due to changes in the pathways of the cranial nerves.
Branches of the facial nerve are affected in alternating syndromes
Syndromes that include sets of symptoms due to ischemia in the area of various nuclei and pathways are called alternating. They accompany truncal paralysis of half the body in different ways, always appear on the affected side, and indicate the level and location of the lesion. Clinical manifestations are named after the doctors who first described these combinations.
Depending on the location, they are divided into syndromes:
- lesions of the cerebral peduncles (peduncular);
- changes in bridge structures;
- disorders in the medulla oblongata (bulbar).
Neurologists are familiar with the descriptions of syndromes and use them in differential diagnosis.
Examples of alternating lesions:
- Millar-Gubler syndrome - paralysis of the facial nerve (drooping of the eyelid, corner of the mouth);
- Brissot-Sicard syndrome - spastic contractions in the area of the branches of the facial nerve;
- Jackson syndrome - paralysis of the hypoglossal nerve with impaired swallowing;
- Avellis syndrome - paralysis of the soft palate and vocal cords, choking when eating, liquid food flowing into the nose, impaired speech;
- Wallenberg-Zakharchenko syndrome - in addition to paralysis of the soft palate and vocal cords, loss of sensitivity on the skin of the face.
Treatment
Treatment of brainstem stroke is carried out from the first hours of detection. Since it is completely impossible to immediately determine the form of the stroke, all prescriptions relate to stabilizing the vital functions of the brain and relieving tissue edema.
To normalize breathing, oxygen therapy is administered through a mask; if breathing is absent or impaired, the patient is intubated and transferred to artificial respiration using a ventilator.
Regulation of cardiac activity requires maintaining blood pressure no higher than 10% of the patient’s normal level; antiarrhythmic drugs are administered, according to indications - cardiac glycosides, nitrates.
To maintain the necessary metabolism, an alkaline solution, preparations with potassium and magnesium are needed.
Reopolyglucin normalizes blood clotting and thickness.
Brain cells are protected with the help of neuroprotective drugs (Cerebrolysin, Piracetam).
To relieve swelling of the brain tissue, magnesium sulfate and diuretics are administered according to indications.
The patient may need symptomatic medications: muscle relaxants, painkillers, anticonvulsants, sedatives. Their administration is determined by the patient’s specific clinic.
The use of such specific agents as thrombolytic therapy is possible only with complete confidence in thrombosis of the cerebral arteries. It is effective only in the first 6 hours of clinical manifestations.
Residual strabismus after trunk stroke
What indicates a negative prognosis?
The consequences of a stroke in the structures of the trunk can be determined in advance after a few days. Neurologists believe that restoration of function is almost impossible with severe bulbar palsy. The patient can live for some time on mechanical breathing, but will die from cardiac arrest.
The presence of the following symptoms indicates a deep impairment of motor functions during paralysis:
- “spread hip” - the femoral part of the paralyzed leg becomes wide and flabby due to loss of muscle tone;
- hypotony of the eyelid - the inability to independently open the eye on the affected side;
- turned foot outward due to atony of the muscles that rotate the leg.
How to predict the prognosis based on stroke symptoms?
Observation of the course of brainstem strokes has led to prognostic assumptions regarding the recovery of patients.
The prognosis is considered unfavorable under the following circumstances:
- speech disorder;
- rare breathing (there is a possibility of a complete stop during sleep);
- tendency to bradycardia and low blood pressure;
- altered thermoregulation (a sharp rise in body temperature, then a drop below normal).
Uncertain prognosis for:
- impaired swallowing (possibly habituation to liquid, pureed food);
- loss of movement in the limbs (recovery should be achieved within a year);
- dizziness;
- uncoordinated eye movements.
In any case, treatment of trunk stroke requires a competent approach to therapy and the use of all rehabilitation opportunities.
I am 39 years old. In January 2015, I had a mixed type stroke in the vertebral basin. I was left with a spending strabismus. What can be used to restore vision? Thank you in advance!
My husband suffered an ischemic stroke in the brain stem (pons on the left), a month and a half passed, but it got worse, he constantly choked while eating and became weaker. We follow all doctor's orders. Walks with a walker with difficulty. The pressure often jumps to 200. I don’t know what to expect. He is 69 years old and of course has type 2 diabetes.
I have a hemorrhagic stroke in the brain stem, I walk staggering, I have constant dizziness, I talk. Doctors said that this is the first time they have seen such a case. Will the dizziness at least go away and when?
My dad had an ischemic stroke of the brain stem on November 17, 2017. Now he has been in a coma for a month after cardiac arrest. EEG shows little brain activity. Please tell me what the forecasts can be in this case?
Cerebrovascular accident in the brain stem
A brainstem stroke is an acute disruption of blood circulation in this area, which is accompanied by the sudden onset of symptoms of neurological deficit that last longer than a day.
In Russia, the incidence rate is 3.3 per 1000 population per year, with most of them being people over 70 years of age. Mortality within the first month from the onset of the disease is 15-25%, and 70% of victims receive disability.
Thanks to the development of medicine, in recent years there has been a trend towards a decrease in the incidence and mortality from strokes. However, there is a “rejuvenation” of this disease.
Most often, stroke strikes older people, but thanks to the development of medicine, mortality is decreasing
To understand what symptoms will occur with this lesion, you need to understand what the anatomical features of the brain stem are.
A little about the structure
The brain consists of the cerebral hemispheres and the brainstem.
Brain structure
The structure of the trunk includes the medulla oblongata, midbrain, diencephalon, and pons.
Brain stem structure
It performs the following functions:
- provides reflexive behavioral activity;
- connects the upper and lower parts of the central nervous system via conductive pathways;
- connects brain structures.
The composition includes gray and white matter. Gray – neurons located in the form of nuclei that have specific functions. White – conductive paths. To distinguish a stroke in the brain stem from others, as well as to accurately determine the location of the lesion, you need to understand the functions of its parts.
Functions of the medulla oblongata:
- Innervation of the muscles of the tongue (nucleus of the XII pair of cranial nerves) and some muscles of the head (nucleus of the XI pair), larynx and oral cavity (nucleus of the IX pair).
- The work of the parasympathetic nervous system (vagus nerve - X pair).
- Maintaining vital functions (breathing, heartbeat) is the core of the reticular formation.
- The implementation of some motor functions is carried out by the extrapyramidal nuclei (oliva).
Bridge functions:
- Conduction of auditory impulses (nuclei of the VIII nerve).
- Providing facial movements, as well as tear and salivation (nuclei of the VII nerve).
- Carrying out the abduction of the eye outwards (nuclei of the VI pair).
- Chewing movements are carried out by the nuclei of the V pair of cranial nerves.
Functions of the midbrain:
- Other movements of the eyeball, eyelids, pupil (IV and III pairs of nerves).
- Regulation of muscle movement and tone (nucleus of the substantia nigra).
- Reflex response to light and sound impulses.
- Muscle sensitivity of the face and neck.
- Coordination of joint rotation of the neck and eyes.
- Collection of sensitive information from internal organs.
The brain stem coordinates the work of all internal organs, reflex activity, and some important motor acts. Depending on the location of the lesion, symptoms will vary.
Etiology
By origin, brainstem stroke occurs:
- ischemic is associated with a lack of blood flow due to blockage (obstruction) of the artery supplying the area;
- hemorrhagic due to rupture of the artery and bleeding from it.
Types of brainstem stroke
The first type is much more common than the second, accounting for 75-80% of all cerebrovascular accidents.
Causes of ischemic stroke
Risk factors for ischemic stroke include old age, high blood pressure, increased cholesterol in the blood, atherosclerosis, smoking, heart disease, and diabetes.
It should be noted that the increase in blood pressure is above 140/90 mm. Hg, relative to normal, doubles the risk of stroke.
All causes of ischemic stroke can be divided into groups:
- Atherothrombotic - ischemia occurs due to a slowly increasing plaque in the area of the vessel. Such a stroke is preceded by symptoms of transient cerebrovascular accident, signs of prolonged “robbing” the brain of oxygen and nutrients: memory loss, absent-mindedness, development of tearfulness or irascibility, and others. More often happens at night or early in the morning.
- Embolic develops suddenly; a sharp and rapid blockage of the afferent artery occurs with an embolus. More often it occurs with heart diseases (atrial fibrillation, defects, artificial valves), which are characterized by the formation of blood clots in the cavities of the heart and their spread through the bloodstream. More often happens during the day, during emotional or physical overload.
- Ischemia may develop with a decrease in blood pressure, when there is insufficient blood flow to the brain. This is a hemodynamic type.
- Lacunar is characterized by damage to small arteries located deep in the brain. It often develops during the day, against the background of high blood pressure. Since small areas are deprived of blood supply, the symptoms are erased, and its prognosis is better than that of others.
- Hemorheological is rare and develops due to increased blood viscosity.
One of the causes of ischemic stroke is high blood pressure
The brain is an organ where chemical processes actively occur, but it does not have its own reserves of nutrients. This means that any reduction in blood flow with oxygen and nutrients quickly affects its function in a negative way. Without a blood supply, a neuron can survive for a maximum of five to eight minutes, after which it dies.
Normally, ml of blood flows through 100 g of brain per minute; with a stroke, this figure drops to 10.
After blockage of a vessel, the following is possible: ischemia occurs in the area it fed, neurons die, and their function is lost. But next to it there is another area (ischemic penumbra or penumbra), in which the blood supply has not reached a dangerous minimum. However, the brain cells in it also suffer from ischemia and damage from the decay products of dead neurons. They are viable, but they are also at risk of death, so it is important to start therapy as early as possible. This will reduce the affected area and preserve more brain functions.
Due to the accumulation of breakdown products, edema develops in this area, which compresses adjacent structures, pushing them to the side, further impairing blood flow and functioning.
Anatomy of ischemic stroke
Causes of hemorrhagic stroke
It occurs less frequently, but its symptoms are more severe and the prognosis is worse. Highlight:
- With parenchymal hemorrhage, changes occur in the substance of the brain. This is possible with arterial hypertension, bleeding disorders or weakness of the vascular wall (aneurysm).
- Subarachnoid - bleeding onto the surface of the brain due to pathology of the vessels in the membranes. More often, it is caused by an aneurysm, so it usually affects young, apparently healthy people.
A brainstem stroke develops when there is a lesion in the vertebrobasilar vascular system.
Symptoms
Brainstem stroke manifests itself in different ways, depending on the location of the lesion. It is characterized by the appearance of alternating (cross) symptoms, that is, the organs of the head and neck are affected on the side of the lesion, and the movements of the limbs and the sensitivity of the skin of the body are affected on the opposite side.
Medulla
If the medulla oblongata is damaged, there will be a complete or partial impairment of the motor function of the tongue (its tip deviates in the direction of the lesion), the muscles of the soft palate, neck, vocal cords (hoarseness) on the side of the stroke, and loss of sensitivity of the facial skin. On the opposite side there is a violation or inability to move the arms or legs, numbness of half the body.
Stroke has a poor prognosis in the presence of bulbar palsy. It develops when blood circulation in the vertebral arteries is impaired, which causes bilateral damage to the IX, X, XII pairs of cranial nerves located in the medulla oblongata. In this case, such disorders as choking when swallowing, overhanging soft palate, impaired diction, hoarseness of voice, small twitching of the tongue and limited mobility are noted. It is often followed by impairment of vital functions and death.
If the pathological focus is in the bridge, then on the affected side there is an inability to move the facial muscles, loss of superficial sensitivity on the face, decreased hearing, the gaze is directed towards the focus. On the opposite side, motor disturbances in the limbs and decreased sensitivity are detected. Often accompanied by impaired consciousness up to coma.
Pseudobulbar palsy manifests itself in the same way as bulbar palsy, but its cause is damage to the pathways at the level of the pons and above, so the prognosis is more favorable, since disturbances in vital functions usually do not follow. A distinctive feature is the absence of tongue twitching, the pharyngeal and palatal reflexes are preserved or increased, and symptoms of oral automatism are detected.
With thrombosis of the basilar artery, “locked-in syndrome” develops. While consciousness is preserved, the patient does not move any muscles except the eyeballs and blinking.
Midbrain
A brainstem stroke localized in the midbrain is manifested by the inability to make eye movements and lack of pupillary response on the affected side. On the opposite side, the movement of the limbs is disrupted, and tremor (involuntary shaking) of the hand appears. Pseudobulbar palsy may develop.
Decerebrate and decortication rigidity syndrome indicates a poor prognosis. The cause is a brainstem stroke in the area of the midbrain pathways at a level above the vestibular nuclei. Decerebrate rigidity is manifested by coma in combination with an increase in the tone of all muscles, mainly extensors, when the arms and legs are brought to the body and the head is thrown back. Decortication - the upper limbs are bent and the lower limbs are extended.
If the lesion is localized below the vestibular nuclei, then coma occurs with a lack of muscle tone.
Diagnostics
If a brainstem stroke is suspected, as with other lesions, magnetic resonance or computed tomography is performed, if possible. This makes it possible to identify the presence and location of an area of impaired blood circulation. The speed of correct diagnosis directly affects the final prognosis of the disease.
Doppler ultrasound is a technique for studying blood flow in vessels. It identifies areas of missing blood supply or hemorrhage.
An important indicator of the functional characteristics of the body are general clinical tests (general blood and urine analysis), biochemical blood test, ECG, and, if necessary, EchoCG (visual ultrasound examination of the heart).
All this information allows us to establish the diagnosis of stroke, its localization, which determines the prognosis of recovery and treatment tactics.
Treatment
If a stroke of any localization is suspected, hospitalization in the neurological department is required.
If you suspect a stroke, seek medical attention
Trunk stroke is treated according to the same principles as any other. Basic therapy includes maintaining vital body functions: breathing, blood pressure, heartbeat, body temperature, as well as reducing cerebral edema.
Specific therapy is aimed at eliminating the causes of the disease. This includes, for example, thrombolysis, normalization of blood viscosity. Measures are being taken to provide neuroprotection and restore neuronal function.
The faster the symptoms of neurological deficit pass, the better the future prognosis.
Consequences
Unfortunately, brainstem stroke often has an unfavorable prognosis. The patient remains with dizziness, speech and swallowing disorders, muscle paralysis of various locations and functions, and loss of sensitivity for a long time.
Rehabilitation aimed at replacing these functions is long-term and permanent, and the improvements that occur are slow and insignificant.
However, this does not mean that you need to give up rehabilitation. Recovery is possible only by working on impaired functions.
- Musaev on Duration of treatment for meningitis
- Yakov Solomonovich on Consequences of stroke for life and health
- Permyarshov P. P. on Life expectancy for a cancerous brain tumor
Copying site materials is prohibited! Reprinting of information is permitted only if an active indexed link to our website is provided.
Brain stem tumor: signs, treatment tactics and survival prognosis
Brain stem tumors are one of the diseases of the central nervous system, manifested by many symptoms. The medulla oblongata and midbrain are affected.
In 90% of situations, the disease is of glial origin. Glia are cells that create the necessary conditions for the full functioning of the central nervous system.
Statistics
There are 20 people with this diagnosis per 100 thousand population. The disease develops in people of different ages, races, and genders.
A malignant tumor has ICD-10 code C71.7.[
Brainstem tumors affect nuclear formations and pathways, but rarely cause disruption of the outflow of cerebrospinal fluid. The latter occurs only in advanced stages and when developing near Sylvian aqueducts.
Varieties
Neoplasms affecting the trunk are divided into benign and malignant.
The first type is characterized by a slow increase. Sometimes this takes more than 15 years. Malignant ones lead to rapid death.
Despite the fact that tumors are localized in different areas, they most often affect the bridge.
Stem tumors are divided into:
- Primary stem, formed according to the intra-stem or exophytic type. They are formed only from the tumor of the table itself.
- Secondary stem, emerging from other brain structures. They develop from the cerebellum, the fourth ventricle, and only over time grow into the trunk.
- Para-stem formations lead to deformation of the trunk or are simply in close interaction with it.
Tumors are also classified according to their growth characteristics. If they take development from their own cells and form a shell, pushing aside tissue, then we are talking about expansive growth. If the neoplasm grows into other tissues, it is called infiltrating. In a diffuse tumor of the brain stem, which occurs in 80% of cases, the boundaries of the tumor are not determined even microscopically.
Causes
The exact prerequisites for the appearance remain hidden, but experts focus on hereditary factors and receiving high doses of ionizing radiation.
In the first case, the genetic information of the cells changes. This leads to the fact that they begin to have tumor properties, multiply uncontrollably and inhibit the vital activity of other cells.
Those people who have previously received radiation treatment for dermatomycosis of the scalp have a predisposition to neoplasms.
Today this method is not used, but modern methods of radiation therapy also lead to the formation of malignant cells.
There are suggestions that vinyl chloride causes brain stem cancer. This gas is used in the production of plastic.
Symptoms of brain stem tumors in adults and children
There are many structures in the brain stem, so the course of the disease can vary. In children, due to the development of compensatory mechanisms of nervous tissue, neoplasms often have a long-term asymptomatic course.
Further symptoms depend on the location of the tumor and the type of tumor. In adults, focal symptoms are difficult to identify.
In preschool children, the first alarming signs are loss of appetite, decreased mental and motor activity. Schoolchildren experience a significant decline in academic performance, changes in behavior, and the appearance of chronic fatigue. A movement disorder almost always occurs.
As the tumor grows, symptoms increase. Frequent migraines, nausea, vomiting are added. The disturbances affect the cardiovascular and respiratory centers of the trunk. This is what causes death.
The emergence of new behavioral reactions is noted
If the neoplasm is malignant, convulsions and fear of light occur.
Diagnosis of neoplasms
The study involves carrying out a full range of diagnostic measures. A preliminary diagnosis is established by a neurologist.
The main importance is given to:
- Computed tomography, which makes it possible to obtain information about the composition of tissues, identify pathologies and carry out monitoring over time. During the procedure, images of brain slices at different levels are obtained.
- SCT is a method that allows ultra-fast scanning of structures, therefore it is used for patients in serious condition. Allows you to record even the smallest deviations in the structure.
- MRI with contrast agent injection. This method reveals small formations and makes it possible to determine the presence of an exophytic component. This also allows for a preliminary assessment of the presence of tumor growth and the degree of infiltration.
Thanks to these techniques, a brain stem tumor is differentiated from multiple sclerosis, encephalitis, stroke, and hematoma.
Additionally, angiography is performed. The method is necessary to determine the specifics of the blood supply to the formation and the vessels feeding the tumor. A biopsy is performed to obtain samples of the tumor. The procedure is performed using minimally invasive surgical methods using ultrasound or X-ray guidance.
Treatment of pathology
Only a radical integrated approach, consisting of:
The first technique is aimed at removing the formation while preserving as much healthy trunk tissue as possible. Surgical intervention becomes possible after performing a craniotomy, that is, making an opening in a pre-selected location to gain access to the tumor.
Radiation therapy can also be performed in situations where surgical treatment is contraindicated. The method is not recommended for children under three years of age, as physical and intellectual retardation develops later. To carry out the procedure, special installations are used that allow the tumor to be exposed from different angles.
This direction is called stereotactic radiosurgery. First, a study is conducted to accurately determine the location. Then irradiation is carried out using special equipment.
Chemotherapy is aimed at suppressing the growth of malignant cells. For this purpose, medications are used that act on formations, causing a minimum of side effects. This method can also be used for children who have not yet reached three years of age.
Most drugs are administered intravenously into the blood using droppers and injections. Sometimes the doctor decides to give medications through a long tube that connects to a large vein in the chest. Chemotherapy is carried out cyclically.
Disease prognosis
It is believed that when a brain stem tumor is removed in childhood, the prognosis is several times better than in adults.
Benign tumors can grow for up to 15 years without symptoms, but most tumors in the brain stem are malignant.
In this case, death occurs within several years or months from the onset of symptoms. Typically, treatment only slightly prolongs life.
What is a brainstem infarction?
In fact, the trunk is nothing more than a “bridge” connecting the spinal cord to the brain. It is he who is responsible for transmitting all the “orders” of the brain throughout the body.
Brainstem infarction is accompanied by damage to the cerebellum, thalamic region, medulla oblongata and midbrain, and pons.
In this area are also located the nuclei of the cranial nerves, which “guide” the contraction of the muscles of the eyes, face, and also the muscles that help make swallowing movements. The trunk also contains the most important centers for human life, which are responsible for respiratory function, thermoregulation, and blood circulation.
- All information on the site is for informational purposes only and is NOT a guide to action!
- Only a DOCTOR can give you an ACCURATE DIAGNOSIS!
- We kindly ask you NOT to self-medicate, but to make an appointment with a specialist!
- Health to you and your loved ones!
A cerebral infarction is a hemorrhage in the brain followed by the formation of a hematoma that cuts off the supply of oxygen to the damaged area.
As a result of the development of hypoxia, that is, lack of oxygen, atrophy of the brain stem occurs, which leads to disruption of the functioning of all internal organs.
Depending on the mechanism by which the lesion develops, ischemic and hemorrhagic infarction are distinguished. Currently, the first, according to mortality statistics, ranks second. It is also called cerebral infarction.
An ischemic heart attack is an extensive damage to brain tissue caused by a serious disruption in blood circulation. Blood simply does not reach certain areas of the brain, which leads to softening and death of tissue in them.
The causes of brainstem infarction are varied, but the main one is atherosclerosis. It can also develop due to diabetes mellitus, and in some cases due to rheumatism and hypertension.
When a patient experiences decreased motor activity, dizziness, problems with coordination, and nausea, all this indicates the development of an ischemic heart attack.
Symptoms
Hemorrhage, or the so-called infarction of the brain stem region, occurs suddenly. As a rule, this is accompanied by dizziness, blurred speech, the occurrence of autonomic disorders, such as a decrease and then an increase in body temperature, redness or pallor of the face, and sweating.
Pulse tension and increased blood pressure are also observed. Further, circulatory and respiratory problems are added to this list of symptoms. A cerebral infarction can be suspected by the occurrence of rapid, infrequent breathing, complicated by exhalation and inhalation.
Sometimes, against the background of a cerebral infarction, some patients experience “locked-in person” syndrome - due to a disruption in the distribution of electrical impulses from the brain throughout the body, the patient experiences paralysis of the limbs.
At the same time, the intellectual ability and ability to evaluate and understand what is happening around remains. These patients can actively help during their recovery.
When a cerebral infarction occurs, 2/3 of all cases end in death in the first two days due to damage to the most basic vital functions of the body. If medical care is provided in a timely manner, death can be avoided. A favorable outcome can also occur if brainstem infarction occurs in young people.
When the first signs of a heart attack appear, even minor ones, you should immediately call an ambulance or consult a doctor.
Prognosis for dysfunction
The prognosis for brain stem infarction is very disappointing. 30% of patients experience speech problems. She becomes inarticulate, quiet and incomprehensible. However, this problem can be slightly solved by using the services of a speech therapist. In the case of the development of “locked-in person” syndrome, such a solution to the problem is impossible, since patients can only move their eyelids.
- Most often, with a cerebral infarction, disruptions in the swallowing function occur (according to statistics, about 65%);
- for patients with dysphagia, i.e. with inflammatory processes in the pharynx or mouth, the prognosis for recovery is uncertain;
- The only option is to re-teach patients to swallow ground or soft food using various techniques.
- when a truncal infarction occurs, patients experience a malfunction of the limbs, and they begin to move spontaneously;
- a positive prognosis for such a function is possible only in the first 2-3 months;
- in the future, the more time passes from the moment of illness, the more recovery decreases;
- sometimes the recovery process can last for a year;
- longer periods are extremely rare.
- if during a trunk infarction the respiratory section is affected, then patients are simply unable to breathe on their own;
- unfortunately, the prognosis for them is very disappointing: their life will completely depend on the artificial respiration apparatus;
- if the respiratory center is not completely damaged, then patients may experience sleep apnea;
- this is nothing more than stopping breathing during sleep for a short period;
- Slow breathing may also occur while you are awake.
- the earliest sign indicating that a cerebral infarction has occurred is dizziness;
- as a rule, this symptom goes away quite quickly with proper treatment and recovery;
- The time until the symptom completely disappears is uncertain and depends solely on how severely the brain was affected.
- a heart attack of the trunk can also lead to a malfunction of the cardiovascular system;
- in this case, rapid heartbeat and increased blood pressure are observed;
- when the heart rate decreases, the prognosis for the patient is, alas, unfavorable;
- in this case, the patient is in a serious condition, which can be fatal.
- Also, with a heart attack of the trunk, thermoregulation may be affected, indicating a serious condition of the patient;
- as a rule, there is a rise in temperature to 39 degrees or more on the first day of a heart attack;
- this condition is difficult to regulate;
- if the patient’s body temperature is lowered, this indicates that the brain cells will soon die.
- Quite often, a heart attack affects the visual center located in the brain stem;
- therefore, the patient may experience spontaneous eye movement (either one or both);
- a person’s ability to focus his gaze on some object or image is also impaired, it becomes difficult to move his eyes up and to the sides, and strabismus may develop.
Read about the consequences and rehabilitation after large-focal myocardial infarction in another publication.
Brainstem infarction requires professional and long-term treatment. In severe conditions, it may require surgery.
Treatment of brainstem infarction
As mentioned above, even if a cerebral infarction is suspected, the patient must be urgently taken to the hospital. The very first task that needs to be solved is to stop blood circulation in the brain, including the affected part, and also to normalize the functioning of the lungs and heart.
In severe cases of cerebral infarction, surgical intervention is performed. As a rule, it is carried out in the first hours after the onset of an attack.
Unfortunately, quite often the infarction of the trunk is so severe that it does not allow the use of angiographic examination or even surgery. In this case, doctors carry out the necessary resuscitation measures.
Patients with brainstem infarction, even after surgery, require long-term treatment and rehabilitation therapy in order to reduce and eliminate possible consequences.
To prevent a recurrent attack, it is necessary to promptly treat chronic heart and vascular diseases, as well as regulate atherosclerotic processes by changing the diet.
For the treatment of brainstem infarction, the following are usually prescribed:
- physiotherapy;
- medications that prevent the formation of blood clots in blood vessels;
- medications that lead to blood thinning, and, consequently, blood clots;
- medications aimed at reducing blood pressure;
- medications that lower blood cholesterol levels;
- medicines that help control heart rhythm.
Trunk infarction is one of the diseases that is very difficult to treat. Recently, quite often one of the methods of treating this disease is the infusion of platelets into the area of the brain damaged by the infarction.
Rehabilitation therapy can be carried out both at home and in rehabilitation centers or specialized sanatoriums
Treatment also includes resuscitation, inpatient therapy and physical therapy.
Read here about intramural myocardial infarction.
You will find a description of focal infarction in this article.
During the treatment period, it is very important to eliminate all physical and emotional stress on the body, as well as maintain all its important life support functions. This approach allows you to very quickly restore blood circulation in the affected area of the brain.
The next stage of treatment is rehabilitation therapy. You should not postpone it for a long time, as this leads to the loss of certain brain functions, which, unfortunately, will then be impossible to restore.
Oculolethargic syndrome. Predominant damage to the oral parts of the trunk (nuclei of the oculomotor nerves), the hypothalamic region and the reticular formation of the trunk.
Damage to the left nucleus of the spinal tract.
Segmentally dissociated type of sensitivity disorder. Oral parts of the nucleus of the spinal tract of the trigeminal nerve (pons) on the left.
Alternating Weber syndrome. Damage to the brain stem, mainly the base of the midbrain (peduncle) on the right.
Alternating syndrome. Damage to the brain stem, mainly the pons on the right.
Alternating Millard-Gubler syndrome. Damage to the lower part of the bridge on the right.
Alternating Jackson syndrome. Medulla oblongata on the right.
Pseudobulbar palsy. Bilateral damage to the corticobulbar tract (more pronounced on the right).
Bulbar palsy. Predominant damage to the tegmentum of the brain stem at the level of the nuclei of the 12th, 9th, 10th cranial nerves (medulla oblongata).
4. Damage to the cerebellum
Right hemisphere of the cerebellum.
5. DAMAGE TO THE SUBCORTICAL NODES
Lesion of the left visual thalamus.
Parkinsonism syndrome. Predominant damage to the pallidal system (globus pallidus, substantia nigra).
Choreic hyperkinesis syndrome. Predominant damage to the striatal system (putamen, caudate nucleus).
6. DAMAGE TO THE HYPOTHALAMIC-PITITUITARY AREA
Hypothalamic-pituitary syndrome. Predominant damage to the pituitary gland.
Sympathetic-adrenal crisis. Predominant damage to the hypothalamus (diencephalic region).
Itsenko-Cushing syndrome. Damage to the pituitary-hypothalamic region.
7. DAMAGE TO THE INTERNAL CAPSULE
Central palsy of the facial and hypoglossal nerves. Internal capsule on the right.
8. DAMAGE TO THE LOBE, GYRIUS OF THE BRAIN
Predominant damage to the frontal lobe on the left.
Lesion of the left frontal lobe.
Predominant damage to the frontal lobe on the left (with symptoms of irritation of the second frontal gyrus).
Motor Jacksonian epilepsy. Lesion of the right precentral gyrus.
Apraxia syndrome (motor, constructive). Damage to the left parietal lobe, mainly the supramarginal and angular gyri.
Disorders of muscle-joint, tactile sensitivity, sense of localization in the left hand, disorder of the “body diagram”. Damage to the right parietal lobe, mainly the superior parietal lobule and interparietal sulcus.
Predominant damage to the left temporal lobe.
9. Task-schemes
Quadrant hemianopsia (lost lower left quadrant).
Left-sided hemianopsia with preservation of the central visual field.
Visual agnosia.
Astereognosia, apraxia.
Sensory aphasia.
Amnestic, semantic aphasia.
Gustatory, olfactory agnosia.
Quadrant hemianopsia (the right upper quadrant has fallen out).
Lateral pyramidal tracts at the level of the cervical segments.
The anterior horns of the spinal cord or anterior roots at the level of segments C 5 -C 8 on the right.
Damage to the nucleus of the facial nerve on the left (pons) and the lateral pyramidal tract at the same level (alternating paralysis)
The lesion is on the right (cerebral peduncle, internal capsule, corona radiata, anterior central gyrus). Hemiplegia on the left.
Multiple lesions of peripheral nerves (polyneuritis).
The anterior horns of the spinal cord and the lateral pyramidal tract on the left at the level of segments C5-C7.
The anterior horns of the spinal cord or the anterior roots of the spinal nerves at the level of segments L 1 -S 1 on both sides.
Lateral pyramidal tract at the level of segment D 12 on the left or the upper part of the right precentral gyrus.
Bilateral damage to the lateral pyramidal tracts at the level of segments D 9 - D 10 or the upper parts of the precentral gyri.
The anterior horns of the spinal cord at the level of segments C 5 -C 8 and the lateral pyramidal tracts at the same level on both sides.
Internal capsule or thalamus, or corona radiata, or postcentral gyrus. The hearth is on the left.
Multiple lesions of the peripheral nerves of the extremities (polyneuritic type of sensitivity disorder).
Posterior columns of the spinal cord at the level of segment D 4 (Gaull's bundles).
Posterior horns at the level of segments C 5 - D 10 on the right.
The posterior column of the spinal cord and the lateral spinothalamic tract on the right at the level of segments D 5 - D 6.
Lateral spinothalamic tract and deep sensory pathways (medial lemniscus) at the level of the brain stem (pons), sensory nuclei of the trigeminal nerve, ibid.
Lateral spinothalamic tract at the level of segments D 8 - D 9 on the left.
Right brachial plexus.
Spinal nerve roots at the level of segments S 3 -S 5 on both sides:
Lateral spinothalamic tracts on both sides at the level of segments D 10 - D 11 and the posterior cords of the spinal cord at the same level.
Lateral pyramidal tract at the level of segment D 10 on the right, spastic paresis of the right leg, absence of middle and lower abdominal reflexes on the right.
Anterior horns of the spinal cord at the level of segments L 2 -L 4 on both sides. Peripheral paralysis of the lower extremities (mainly thigh muscles).
Anterior roots of the spinal nerves at the level of segments L 4 -S 1 on both sides. Peripheral paralysis of the muscles of the legs and feet.
Anterior roots of the spinal nerves at the level of segments C 5 -C 8 on the right. Peripheral paralysis of the right arm.
Anterior horns of the spinal cord at the level of segments L 1 -L 2 on both sides. Peripheral paralysis of the thigh muscles.
Lateral pyramidal path at the level of segments L 2 -L 3. Spastic paralysis of the lower limb.
Lateral pyramidal tract at the level of segment D 5 on the left. Spastic paresis of the left leg, absence of abdominal reflexes on the left.
Anterior horns of the spinal cord at the level of segments C 1 - C 4 on the left.
Anterior horns of the spinal cord and lateral pyramidal tracts on both sides at the level of segments C5-C8. Peripheral upper and central lower paraparesis, urinary and fecal retention.
Anterior horns of the spinal cord, lateral pyramidal tract on the right at the level of segments L 1 -L 2. Peripheral paresis of the muscles of the thighs, central paresis of the muscles of the leg and foot on the right.
Anterior horns of the spinal cord at the level of segments C 5 -C 8 on the left. Peripheral paralysis of the left arm.
The anterior horns of the spinal cord and the lateral pyramidal tract on the right at the level of segments C5-C8. Peripheral paresis of the right arm with fibrillations, central paresis of the right leg. Peripheral paralysis of the neck muscles, paralysis of the diaphragm.
Lateral pyramidal tract on the left at the level of segment D 12. Spastic paralysis of the lower limb while maintaining the upper and middle abdominal reflexes.
Anterior roots of the spinal nerves at the level of segments S 3 -S 5 on both sides. Peripheral sphincter paralysis (urinary and fecal incontinence). There are no paresis of the limbs.
Lateral pyramidal tract at the level of segment C 5 on the left. Left-sided central hemiparesis.
Lateral spinothalamic tract on the right at level D 10. Conduction disturbance of pain and temperature sensitivity downward from the level of the inguinal fold on the left
Spinal nerves at the level of segments C 5 -C 8 on the left, anesthesia and flaccid paralysis or paresis of the left arm
Brown-Séquard syndrome: central paresis of the left leg and disturbance of deep sensitivity on the left below the axillary region, conduction disturbances of superficial sensitivity on the right.
Transverse lesion of the spinal cord at the level of segment C4. Central tetraplegia, anesthesia of the entire surface of the body; dysfunction of the pelvic organs. Possible paresis of the diaphragm.
The posterior roots of the spinal nerves at the level of segments S 3 -S 5 on both sides. Anesthesia in the area of the external genitalia and anus.
Posterior and anterior roots at the level of segments L 4 - S 1 on the left. Peripheral paresis of the left leg, disturbance of all types of sensitivity.
Facial nerve (central palsy on the left).
Facial nerve (peripheral paralysis on the left).
Oculomotor nerve (ptosis of the right upper eyelid).
Oculomotor nerve (divergent strabismus, mydriasis).
Trigeminal nerve (innervation of the face and head by segments, Zelder zones).
Trigeminal nerve (peripheral innervation of the skin of the face and head).
Hypoglossal nerve (peripheral palsy on the left).
Abducens nerve (when looking to the left, the left eyeball is not diverted outward).
Focal (partial) motor seizure in the right leg.
Adversive seizure (turning the head and eyes to the right)
Auditory hallucination (aura).
Complex visual hallucination (aura).
Simple visual hallucination (aura).
Olfactory, gustatory hallucination (aura).
Motor aphasia (Broca's center).
The head and eyes are turned to the left (gaze paresis), agraphia.
Central paralysis of the right leg.
Brainstem stroke is considered one of the most severe forms of brain damage due to acute disturbance of blood flow. This is no coincidence, because it is in the trunk that the main life support nerve centers are concentrated.
Among patients with brain stem stroke, elderly people predominate, having the corresponding prerequisites for impaired blood flow - hypertension, atherosclerosis, pathology of blood clotting, heart disease, predisposing to thromboembolism.
The brain stem is the most important area, serving as a link between the central nervous system, spinal cord and internal organs. It controls the functioning of the heart, respiratory system, maintaining body temperature, motor activity, regulates muscle tone, autonomic reactions, balance, sexual function, participates in the functioning of the organs of vision and hearing, ensures chewing, swallowing, and contains fibers of taste buds. It is difficult to name a function of our body that would not involve the brain stem.

brain stem structure
The stem structures are the most ancient and include the pons, medulla oblongata and midbrain, sometimes also referred to as. In this part of the brain, the nuclei of the cranial nerves are located and conductive motor and sensory nerve pathways pass. This section is located under the hemispheres, access to it is extremely difficult, and with swelling of the trunk, displacement and compression quickly occur, which are fatal for the patient.
Causes and types of brainstem strokes
The causes of brainstem stroke do not differ from those in other localizations of blood flow disorders in the central nervous system:
- , which causes irreversible changes in the arteries and arterioles of the brain, the walls of the vessels become brittle and sooner or later they may rupture with hemorrhage;
- , observed in the vast majority of older people, leads to the appearance in the arteries supplying the brain, the result is plaque rupture, thrombosis, vessel blockage and necrosis of the medulla;
- and – cause strokes in young patients without or in combination with concomitant pathology.
To a large extent, the development of trunk stroke is facilitated by other metabolic disorders, rheumatism, heart valve defects, blood clotting disorders, including when taking blood-thinning drugs, usually prescribed to cardiac patients.
Depending on the type of damage, brain stem stroke can be ischemic or hemorrhagic. In the first case, a focus of necrosis (infarction) is formed, in the second, blood spills into the brain tissue when a blood vessel ruptures. Ischemic stroke progresses more favorably and with hemorrhagic, edema and intracranial hypertension quickly increase, therefore, mortality is significantly higher in the case of hematomas.
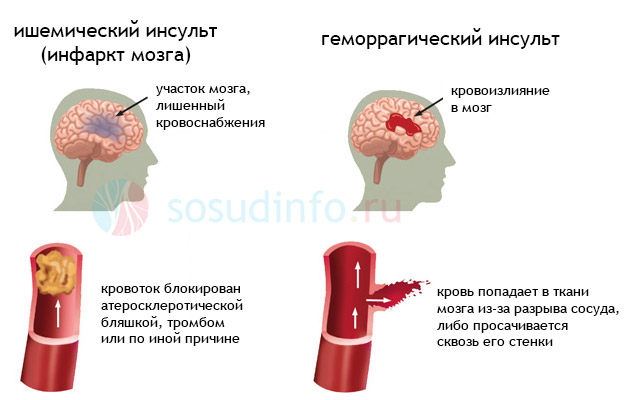
Video: basic about types of stroke - ischemic and hemorrhagic
Manifestations of brainstem damage
A brainstem stroke is accompanied by damage to the pathways and nuclei of the cranial nerves, and is therefore accompanied by rich symptoms and severe disorders of the internal organs. The illness manifests itself acutely, starting with intense pain in the occipital region, impaired consciousness, paralysis, dizziness, tachycardia or bradycardia, and sudden fluctuations in body temperature.
General cerebral symptoms associated with increased intracranial pressure, it includes nausea and vomiting, headache, impaired consciousness, even coma. Then they join symptoms of damage to the cranial nerve nuclei, focal neurological symptoms.

Ischemic brainstem stroke is manifested by a variety of alternating syndromes and signs of involvement of the cranial nerve nuclei of the side where necrosis occurred. In this case, the following may be observed:
- Paresis and paralysis of muscles on the side of the affected part of the trunk;
- Deviation of the tongue towards the affected side;
- Paralysis of the part of the body opposite to the lesion with preservation of the work of the facial muscles;
- Nystagmus, imbalance;
- Paralysis of the soft palate with difficulty breathing, swallowing;
- Drooping of the eyelid on the side of the stroke;
- Paralysis of the facial muscles on the affected side and hemiplegia of the opposite half of the body.
This is only a small part of the syndromes accompanying brainstem infarction. With small lesion sizes (up to one and a half centimeters), isolated disturbances in sensitivity, movements, central paralysis with pathology of balance, hand dysfunction (dysarthria), isolated disturbance in the functioning of the muscles of the face and tongue with speech disorder are possible.
With hemorrhagic brainstem stroke, symptoms increase rapidly In addition to motor and sensory disorders, intracranial hypertension is clearly manifested, consciousness is impaired, and the likelihood of coma is high.
Signs of hemorrhage in the trunk may be:
- Hemiplegia and hemiparesis - paralysis of the muscles of the body;
- Visual impairment, gaze paresis;
- Speech disorder;
- Decreased or absent sensitivity on the opposite side;
- Depression of consciousness, coma;
- Nausea, dizziness;
- Increased body temperature;
- Impaired breathing and heart rhythm.
A stroke usually occurs suddenly and can be witnessed by loved ones, colleagues or passers-by on the street.. If a relative suffers from hypertension or atherosclerosis, then a number of symptoms should alert relatives. Thus, sudden difficulty and incoherence of speech, weakness, headache, inability to move, sweating, fluctuations in body temperature, palpitations should be a reason to immediately call an ambulance. A person’s life may depend on how quickly those around him orientate himself, and if the patient is admitted to the hospital in the first few hours, the chances of saving a life will be much greater.
Sometimes small foci of necrosis in the brain stem, especially those associated with, occur without a sharp change in condition. Weakness gradually increases, dizziness appears, gait becomes uncertain, the patient experiences double vision, hearing and vision decrease, and eating becomes difficult due to choking. These symptoms also cannot be ignored.
Trunk stroke is considered a severe pathology, and therefore its consequences are very serious. If in the acute period it is possible to save life and stabilize the patient’s condition, bring him out of a coma, normalize blood pressure and breathing, then significant obstacles arise at the rehabilitation stage.
After a brainstem stroke, paresis and paralysis are usually irreversible, the patient cannot walk or even sit, speech and swallowing are impaired. There are difficulties with eating, and the patient needs either parenteral nutrition or a special diet with liquid and pureed food.
Contact with a patient who has suffered a brainstem stroke is difficult due to speech impairment, but intelligence and awareness of what is happening can be preserved. If there is a chance to at least partially restore speech, then a specialist aphasiologist who knows techniques and special exercises will come to the rescue.
After a heart attack or hematoma in the brain stem, patients remain disabled, requiring constant participation and assistance in eating and performing hygiene procedures. The burden of care falls on the shoulders of relatives, who must be aware of the rules of feeding and handling a seriously ill person.
Complications from brainstem stroke are not uncommon and can cause death. The most common cause of death is considered to be swelling of the brain stem with its pinching under the dura mater of the brain or in the foramen magnum; uncorrectable disturbances in the functioning of the heart and breathing are possible.
In a later period, urinary tract infections, pneumonia, thrombosis of the leg veins, and bedsores occur, which is facilitated not only by neurological deficits, but also by the forced recumbent position of the patient. Sepsis, myocardial infarction, and bleeding in the stomach or intestines cannot be ruled out. Patients with milder forms of brainstem stroke who attempt to ambulate are at high risk of falls and fractures, which can also be fatal.
Relatives of patients with brain stem stroke already in the acute period want to know what the chances of recovery are. Unfortunately, in a number of cases, doctors cannot reassure them in any way, since with this localization of the lesion we are talking about saving lives in the first place, and if the condition can be stabilized, then the vast majority of patients remain deeply disabled.
The inability to correct blood pressure, high, persistent body temperature, coma are unfavorable prognostic signs, in which there is a high probability of death during the first days and weeks after the onset of the disease.
Treatment of brainstem stroke

Trunk stroke is a serious, life-threatening condition that requires immediate treatment; the prognosis of the disease largely depends on how quickly treatment is started. All patients, without exception, must be hospitalized in specialized departments, although in some regions this figure is terribly small - about 30% of patients are admitted to hospital on time.
The optimal time to start treatment is considered to be the first 3-6 hours from the onset of the disease, while even in large cities with high availability of medical care, treatment is often started after 10 or more hours. is performed on single patients, and round-the-clock CT and MRI is more a fantasy than a reality. In this regard, forecast indicators continue to remain disappointing.
A patient with a brainstem stroke should spend the first week in the intensive care unit under the constant supervision of specialists. When the acute period is over, transfer to the early rehabilitation ward is possible.
The nature of therapy has specific features for ischemic or hemorrhagic types of lesions, but there are some general principles and approaches. Basic treatment is aimed at maintaining blood pressure, body temperature, lung and heart function, and blood constants.
To maintain lung function you need:
- Sanitation of the upper respiratory tract, tracheal intubation, artificial ventilation;
- Oxygen therapy for low saturation.
The need for tracheal intubation during a brainstem stroke is associated with impaired swallowing and cough reflex, which creates the preconditions for stomach contents to enter the lungs (aspiration). Blood oxygen is controlled by, and its oxygen saturation (saturation) should not be lower than 95%.
When the brain stem is damaged, there is a high risk of cardiovascular disorders, so the following is necessary:
- Blood pressure control - ;
- ECG monitoring.
Even for those patients who did not suffer from arterial hypertension, antihypertensive drugs are indicated to prevent recurrent stroke. In addition, if the pressure exceeds 180 mm Hg. Art., the risk of worsening brain disorders increases by almost half, and a poor prognosis by a quarter, which is why it is so important to constantly monitor blood pressure.
If the pressure was high before the brain damage, then maintaining it at a level of 180/100 mmHg is considered optimal. Art., for people with initial normal blood pressure – 160/90 mm Hg. Art. Such relatively high numbers are due to the fact that when pressure drops to normal, the degree of blood supply to the brain also decreases, which can aggravate the negative consequences of ischemia.

Used to correct blood pressure labetalol, captopril, enalapril, dibazol, clonidine, sodium nitroprusside. In the acute period, these drugs are administered intravenously under pressure control, and later oral administration is possible.
Some patients, on the contrary, suffer from hypotension, which is very detrimental to the affected part of the brain, because hypoxia and neuronal damage increase. To correct this condition, infusion therapy with solutions is performed ( rheopolyglucin, sodium chloride, albumin) and use vasopressor drugs ( norepinephrine, dopamine, mesatone).
Monitoring of biochemical blood constants is considered mandatory. So, when the sugar level decreases, glucose is administered, and when the sugar level increases by more than 10 mmol/l, insulin is administered. In the intensive care unit, sodium levels, blood osmolarity, and the amount of urine excreted are constantly measured. Infusion therapy is indicated when the volume of circulating blood decreases, but at the same time, a slight excess of diuresis over the amount of infused solutions is allowed as a measure to prevent cerebral edema.
Almost all patients with brain stem strokes have an elevated body temperature, because the thermoregulation center is located in the affected part of the brain. The temperature should be reduced starting from 37.5 degrees, for which they use paracetamol, ibuprofen, naproxen. A good effect is also obtained when administered into a vein. magnesium sulfate.
The most important step in the treatment of brainstem stroke is the prevention and control of cerebral edema, which can lead to displacement of the median structures and their wedging into the foramen magnum, under the tentorium of the cerebellum, and this complication is accompanied by high mortality. To combat cerebral edema, use:
- Osmotic – glycerin, mannitol;
- Administration of albumin solution;
- Hyperventilation during mechanical ventilation;
- Muscle relaxants and sedatives (pancuronium, diazepam, propofol);
- If the measures listed above do not bring results, barbiturate coma and cerebral hypothermia are indicated.
In very severe cases, when it is not possible to stabilize, muscle relaxants, sedatives are used simultaneously and artificial ventilation is established. If this does not help, surgical intervention is performed - hemicraniotomy aimed at decompressing the brain. Sometimes the ventricles of the brain are drained - in case of hydrocephalus with an increase in pressure in the cranial cavity.
Symptomatic therapy includes:
- Anticonvulsants (diazepam, valproic acid);
- Cerucal, motilium for severe nausea, vomiting;
- Sedatives – Relanium, haloperidol, magnesia, fentanyl.
Specific therapy for ischemic stroke consists of performing thrombolysis, administering and restoring blood flow through a thrombosed vessel. Intravenous thrombolysis should be carried out in the first three hours from the moment of blockage of the vessel; alteplase is used.
Antiplatelet therapy consists of prescribing aspirin; in some cases, the use of anticoagulants (heparin, fraxiparin, warfarin) is indicated. To reduce blood viscosity, it is possible to use rheopolyglucin.
All of the listed methods of specific therapy have strict indications and contraindications, so the advisability of their use in a particular patient is decided individually.
Needed to restore damaged brain structures. For this purpose, glycine, piracetam, encephabol, cerebrolysin, emoxypine and others are used.
Specific treatment hemorrhagic strokes consists of the use of neuroprotectors (mildronate, emoxipine, Semax, nimodipine, actovegin, piracetam). Surgical removal of the hematoma is difficult due to its deep location, but stereotactic and endoscopic interventions have advantages, minimizing surgical trauma.
The prognosis for a brainstem stroke is very serious, the mortality rate for heart attacks reaches 25%, and with hemorrhages, more than half of the patients die by the end of the first month. Among the causes of death, the main place belongs to cerebral edema with displacement of stem structures and their infringement in the foramen magnum, under the dura mater. If it is possible to save the life and stabilize the patient’s condition, then after a brainstem stroke he will most likely remain disabled due to damage to vital structures, nerve centers and pathways.
Brain stem(truncus encephali; synonym brain stem) - part of the base of the brain containing the nuclei of the cranial nerves and vital centers (respiratory, vasomotor and a number of others). The brain stem is about 7 cm long, consists of the midbrain, pons (pons) and medulla oblongata and is located behind the slope of the internal base of the skull to the edge of the foramen magnum. Extends between the cerebral hemispheres and the spinal cord.The midbrain (mesencephalon) is formed ventrally by the left and right cerebral peduncles, dorsally by the quadrigeminal region, consisting of the superior and inferior colliculi; Cranially it borders with the diencephalon, caudally passes into the pons, and through the superior cerebellar peduncles it connects with the cerebellum. The third and fourth pairs of cranial nerves emerge from the midbrain.
The pons - the middle thickened part of the brain stem - forms the middle cerebellar peduncles in the dorsolateral direction and borders caudally with the medulla oblongata.
The ventral surface of the medulla oblongata is formed by the pyramids and the olives lying dorsolateral to them. On the dorsal surface of the medulla oblongata, wedge-shaped and gentle tubercles and the lower cerebellar peduncles are distinguished. The dorsal surface of the pons and medulla oblongata forms the bottom of the IV ventricle - the rhomboid fossa. The V-VIII pairs of cranial nerves emerge from the pons, and the IX, X, XII pairs emerge from the medulla oblongata.
In transverse sections of the brainstem in the ventrodorsal direction, the base, tegmentum, parts of the ventricular system (the midbrain aqueduct and the fourth ventricle), the roof of the midbrain (quadrigeminal) and the roof of the fourth ventricle are distinguished. The base is represented by the bases of the cerebral peduncles, the ventral part of the pons and the pyramids of the medulla oblongata, formed by fibers of the motor tracts: cortical-cerebellar and pyramidal. The tegmentum consists of the nuclei of the cranial nerves (III-XII pairs), the reticular formation, sensitive ascending tracts, nuclei and pathways of the extrapyramidal system.
The motor and parasympathetic nuclei of the cranial nerves are located in the medial part of the tegmentum. The nuclei of the nerves of the muscles of the eyeball (III, IV, VI pairs), as well as the innervating muscle of the tongue (XII pairs) are located near the midline, ventral to the cerebral aqueduct and the bottom of the IV ventricle. The parasympathetic nuclei of the VII, IX and X cranial nerves (superior and inferior salivary, dorsal nucleus of the vagus nerve) lie lateral to the motor ones, and the accessory oculomotor nucleus (accommodation center) occupies a dorsal position in the complex of nuclei of the III pair. The motor nuclei of the nerves of the visceral arches (V, VII, IX, X pairs) lie ventral to the parasympathetic nuclei of the trunk and innervate the masticatory and facial muscles, the muscles of the pharynx and larynx.
The sensitive nuclei of the trunk occupy the side parts of the tire. The nucleus of the solitary tract (VII, IX and X pairs), located in the medulla oblongata, receives interoceptive impulses from the taste buds of the tongue, the mucous membrane of the pharynx, larynx, trachea, bronchi, esophagus and stomach, from the receptors of the lungs, carotid corpuscle, aortic arch and right atria. The pontine and spinal nuclei of the V pair receive exteroceptive impulses from the scalp and face, the conjunctiva of the eyeball, from the mucous membrane of the mouth, nose, paranasal sinuses and tympanic cavity. The midbrain nucleus of pair V receives impulses from the proprioceptors of the head muscles. The cochlear and vestibular nuclei receive impulses from the organ of Corti and the statokinetic apparatus through the VIII pair of cranial nerves.
The reticular formation, which lies between the nuclei of the cranial nerves and the pathways, passes caudally into the intermediate substance of the spinal cord and rostally reaches the subthalamic region and the intralamellar nuclei of the thalamus. The lateral (sensory and associative) and medial (effector) parts of the reticular formation, together with the nuclei of the cranial nerves, form complex functional systems (respiratory and vasomotor centers), regulate muscle tone and ensure the maintenance of posture, integrate complex reflexes (gag, swallowing), and participate in processing and modulation of primary afferent information (endogenous analgesic system), affect the cerebral cortex (activating ascending system).
The left and right parts of the medulla oblongata are supplied with blood by branches of the vertebral arteries: from the ventral surface - the medial and lateral cerebral and anterior spinal arteries, from the dorsolateral - the inferior posterior cerebellar arteries. Branches of the basilar artery supply blood to the bridge (pontine arteries, cerebral peduncles (midcerebral arteries) and the roof of the midbrain (superior cerebellar and posterior cerebral arteries).
Research methods:
To diagnose brain stem lesions, clinical and instrumental laboratory methods are used. The first group includes neurological studies of the functions of cranial nerves, voluntary movements of the limbs and the coordination of these movements, sensitivity, and autonomic-visceral functions.Instrumental and laboratory methods include spinal puncture, suboccipital puncture followed by laboratory examination of cerebrospinal fluid, skull radiography, pneumoencephalography, ventriculography, rheoencephalography, Doppler ultrasound, echoencephalography, electroencephalography (with evoked potentials), which allows recording the bioelectrical activity of certain areas of the brain stem; radionuclide studies, computed tomography and nuclear magnetic resonance imaging, which make it possible to visualize the pathological focus, clarify its nature and prevalence.
Pathology:
The variety of clinical manifestations of brain stem damage depends on the location and size of the focus of the pathological process. The most common topical diagnostic signs of midbrain damage are alternating syndromes, various oculomotor disorders, disorders of consciousness and sleep, and decerebrate rigidity. When the lesion is localized at the base of the midbrain, conduction disorders predominate. Alternating Weber syndrome develops, characterized by damage to the oculomotor nerve on the side of the lesion and hemiplegia with central paresis of the muscles of the face and tongue on the opposite side.Sometimes, with vascular lesions of the midbrain, a syndrome occurs due to simultaneous damage to the superior cerebellar peduncle, spinothalamic tract and quadrigeminal tract, with choreiform hemiathetoid hyperkinesis observed on the side of the lesion and a disorder of pain and temperature sensitivity on the opposite side.
Lesions of the nuclei of the oculomotor nerve cause drooping of the upper eyelid, limitation of movements of the eyeball up, down, inward, divergent strabismus, double vision, pupil dilation, impaired convergence and accommodation.
When the tegmentum of the midbrain is damaged, upward or downward gaze paralysis develops (impaired function of the posterior longitudinal fasciculus) or vertical pendulum-like movements of the eyeballs, sometimes developing in a state of coma. If the posterior longitudinal fasciculus is damaged, conjugal eye movement may be impaired.
Pathological processes in the midbrain lead to impaired muscle tone. Damage to the substantia nigra causes akinetic-rigid syndrome. When the diameter of the midbrain is damaged at the level of the red nuclei, decerebrate rigidity syndrome may develop. With extensive, often vascular, processes in the midbrain involving the nuclei of the reticular formation, disturbances in wakefulness and sleep often occur. Sometimes “peduncular hallucinosis” is observed, accompanied mainly by visual hallucinations of the hypnagogic type: the patient sees figures of people and animals and maintains a critical attitude towards them.
Unilateral lesions in the pontine region also cause alternating syndromes. When the middle and upper part of the base of the bridge is affected, contralateral hemiparesis or hemiplegia develops; with bilateral damage, tetraparesis or tetraplegia develops. Pseudobulbar syndrome occurs quite often. Millard-Hübler syndrome is characteristic of lesions of the caudal part of the base of the bridge.
A lesion in the caudal third of the pontine tegmentum is accompanied by the development of Foville syndrome: homolateral damage to the VI and VII cranial nerves (in combination with gaze paresis towards the lesion). When the caudal part of the tegmentum is affected, Gasperini syndrome is described, which is characterized by homolateral damage to the V, VI, VII cranial nerves and contralateral hemianesthesia.
With extensive, often vascular, processes in the area of the tegmentum of the brain, occurring with damage to the activating part of the reticular formation, disturbances of consciousness of varying degrees often develop: coma, stupor, stunning, akinetic mutism.
With pathology of the medulla oblongata, the most characteristic is bulbar palsy. Often, lesions of the pyramidal tract at the level of the medulla oblongata cause hemi- or tetraplegia. Often, lesions of the pyramidal tract involve the nuclei and roots of the IX, X, XII cranial nerves, and bulbar alternating syndromes develop.
Damage to the ventral part of the lower half of the medulla oblongata is characterized by the appearance on the side of the lesion of segmental dissociated anesthesia in the caudal dermatomes of Zelder on the face, a decrease in deep sensitivity in the leg and arm, the development of hemiataxia and Bernard-Horner syndrome; on the side opposite to the lesion, conduction hemianesthesia is noted with an upper border at the level of the upper cervical segments.
Damage to the nuclei of the reticular formation is accompanied by respiratory distress (it becomes frequent and irregular), cardiovascular activity (tachycardia, cyanotic spots on the limbs and torso), thermal and vasomotor asymmetry in the acute phase.
Of the pathological processes in the brainstem area, ischemic lesions due to transient cerebrovascular accidents and infarctions as a result of occlusive, usually atherosclerotic, damage to the vessels of the vertebrobasilar system at various levels are more common; hemorrhages developing as a result of arterial hypertension are less often observed. Ischemic lesions of the brain stem are characterized by a scattering of several, usually small, foci of necrosis, which determines the polymorphism of clinical manifestations. With the development of an ischemic focus in the area of the brain stem, along with paresis of the extremities, nuclear damage to the cranial nerves develops (oculomotor disorders, nystagmus, dizziness, dysarthria, swallowing disorders, impaired statics, coordination, etc.), sometimes these symptoms manifest themselves in the form of alternating syndromes.
Brain infarction:
Infarctions in the midbrain region can be primary or secondary, caused by dislocation of the brain with transtentorial herniation during various supratentorial space-occupying processes. The most characteristic of midbrain infarction is the inferior red nucleus syndrome: paralysis of the oculomotor nerve on the side of the lesion, ataxia and intention tremor in the contralateral limbs, sometimes choreiform hyperkinesis is observed. If the oral parts of the red nucleus are damaged, the oculomotor nerve may not be affected.With a heart attack in the medulla oblongata, there are two main options. When the lateral and medial cerebral branches of the vertebral and basilar arteries are blocked, medial medulla oblongata syndrome develops: paralysis of the hypoglossal nerve on the side of the lesion and paralysis of the opposite limbs (Jackson syndrome). When the vertebral and inferior posterior cerebellar arteries are blocked, Wallenberg-Zakharchenko syndrome occurs, which is characterized by paralysis of the muscles of the soft palate, larynx, tongue and vocal muscles on the side of the lesion, on the same side there is dissociated segmental anesthesia of the facial skin, impaired deep sensitivity with selective ataxia in them, cerebellar hemiataxia, Bernard-Horner syndrome. Due to damage to the spinothalamic tract on the opposite side, conduction hemianesthesia is detected.
Clinically, hemorrhages in the brainstem are characterized by disturbances of consciousness and vital functions, symptoms of damage to the nuclei of the cranial nerves, and bilateral paresis of the limbs (alternating syndromes are sometimes observed). Strobism (strabismus), anisocoria, mydriasis, fixed gaze, “floating” movements of the eyeballs, nystagmus, swallowing disorders, bilateral pyramidal reflexes, and cerebellar symptoms are often observed. With hemorrhages in the bridge, miosis and paresis of gaze towards the lesion are noted. An early increase in muscle tone (hormetonia, decerebrate rigidity) occurs with hemorrhages in the oral parts of the brain stem. Lesions in the lower parts of the trunk are accompanied by early muscle hypotonia or atony.
The diagnosis is made based on medical history, clinical manifestations, and additional examination methods. Differential diagnosis must be made with apoplectiform syndrome during myocardial infarction, acute development of a tumor or edema of the brain, traumatic brain injury, hemorrhagic meningoencephalitis, disorders of consciousness of various etiologies.
Therapeutic measures are carried out immediately and differentiated, taking into account the patient’s condition and the nature of the pathological process. Early hospitalization of patients is necessary. Patients in a state of deep coma and with severe impairment of vital functions cannot be transported. Emergency care is aimed at correcting the vital functions of the body: treatment of cardiovascular disorders, respiratory failure (changing the patient’s position, suctioning secretions from the trachea and bronchi; if these measures are ineffective, intubation and tracheostomy), maintaining homeostasis, combating cerebral edema.
The prognosis depends on the nature of the vascular process, its topic, size, and rate of development of complications. The most favorable prognosis is for limited brain stem infarctions in young people.
Rehabilitation includes exercise therapy, massage, classes with a speech therapist, drug therapy using drugs that improve metabolic processes in brain tissue (aminalon, Cerebrolysin, piracetam, etc.).
Infectious lesions of the brain stem:
Infectious lesions of the brain stem are primary and secondary. Among the primary ones, neuroviral lesions are more common than others: poliomyelitis, poliomyelitis-like diseases. In this case, paralysis of the muscles of the face, tongue, pharynx, and larynx is observed. In infectious-allergic processes, for example, the bulbar form of Guillain-Barré polyradiculoneuritis, against the background of a severe general condition and meningeal symptoms, signs of damage to the IX-XII cranial nerves on one or both sides and changes in the cerebrospinal fluid (protein-cell dissociation) appear.The bulbar form of neuroviral diseases is the most dangerous, because often leads to cessation of breathing and cardiovascular activity. Treatment: drugs with antiviral activity (deoxyribonuclease, ribonuclease, interferon), glucocorticoids, detoxification agents (gemodez, neocompensan) and symptomatic, with increasing respiratory failure, artificial ventilation of the lungs is carried out, in the recovery period - drugs that improve metabolism, anticholinesterase drugs, massage, Exercise therapy.
Secondary inflammatory lesions of the brain stem can occur with syphilis, tuberculosis, influenza, etc. In these cases, the nuclear formations of the brain stem, pyramidal tract, sensory conductors, and coordination system are affected.
Inflammatory processes of various nature - encephalitis can cause oculomotor disorders, sleep disturbances, muscle tone disorders, akinetic-rigid syndrome, and occasionally bulbar palsy. Often there is damage to the brain stem in multiple sclerosis, which is expressed by oculomotor disorders, nystagmus and dysfunction of conductive structures, especially the pyramidal tracts.
The medulla oblongata is affected in syringobulbia. In the clinical picture of syringobulbia, the most typical symptom is dissociated sensitivity disorders on the face of a segmental type (decreased sensitivity in the lateral parts of the face). Dizziness, nystagmus, and static ataxia are observed due to damage to the vestibular nuclei in the trunk. Often the nuclei of the bulbar group of cranial nerves are involved in the process; sometimes autonomic crises are observed in the form of tachycardia, respiratory failure, and vomiting. The danger is respiratory distress due to stridor caused by laryngeal paralysis. Treatment is symptomatic.
Amyotrophic lateral sclerosis is characterized by damage to the IX, X, XII pairs of cranial nerves in the brain stem. Disorders of swallowing, articulation, phonation, limitation of tongue movement, atrophy and fibrillary twitching in it appear and increase.
Isolated brainstem injuries are rare and are more often observed with severe traumatic brain injury. In this case, loss of consciousness develops, there may be a deep coma, respiratory and cardiac problems. Symptoms of cerebral ischemia and hypoxia appear with the development of cerebral edema. In some cases, tonic convulsions are possible. With less severe injuries, nystagmus, decreased corneal and pharyngeal reflexes, changes in tendon reflexes and the appearance of pathological reflexes are observed. Emergency care is aimed at correcting respiratory and cardiac disorders. The prognosis depends on the severity of the damage and the completeness of treatment measures.
Brain stem pathology is often caused by intracranial tumors. The clinical picture and symptoms of brain stem lesions due to tumors depend on their location and damage to certain nuclei and pathways.
In the midbrain, the most common are gliomas and teratomas, which first cause internal hydrocephalus due to compression of the cerebral aqueduct, then headache, vomiting, and swelling of the optic discs occur. Damage to the upper part of the midbrain causes upward gaze paresis, combined with convergence paresis (Parinaud's syndrome). Anisocoria and a tendency to dilate pupils are noted. The reaction of the pupils to light, convergence, and accommodation are absent. Weakness and spasticity in the muscles progress. Sensory and cerebellar disturbances are possible.
In the area of the cerebral pons, gliomas are most common; in the medulla oblongata - epindymomas, astrocytomas, oligodendrogliomas, and less commonly, glioblastomas and medulloblastomas. Most often these tumors occur in childhood. The initial signs are focal symptoms caused by damage to the cranial nerves and pathways. Pain in the occipital region appears early, and dizziness often occurs. Diplopia is often the first focal symptom. Early signs may indicate damage to half the trunk.
The diagnosis of a tumor is based on progressive damage to the brain stem and increased intracranial pressure, taking into account these additional research methods. Differential diagnosis is carried out with stroke, multiple sclerosis, encephalitis. Treatment of a brain stem tumor is surgical; if this is not possible, treatment is conservative. The prognosis for intrastem tumors, regardless of their histological structure, is usually unfavorable.